
Health is a crown on the heads of the healthy that only the sick can see.



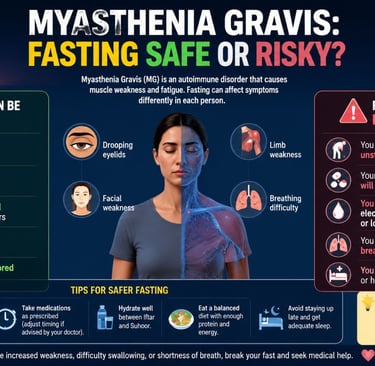
🌙🧠Myasthenia Gravis:Fasting Safe or Risky?
Learn the potential benefits, risks, medication considerations, hydration tips, and expert recommendations for managing myasthenia gravis during fasting.
RESPIRATORY SYSTEMFASTINGAUTOIMMUNE DISEASES
Dr Hassan Al Warraqi
6/7/202615 min read

🌙🧠Myasthenia Gravis:Fasting Safe or Risky?
Learn the potential benefits, risks, medication considerations, hydration tips, and expert recommendations for managing myasthenia gravis during fasting.
gives you key information about MG, based on the medical guidelines.
Always follow the specific advice of your neurologist or MG specialist.
What is Myasthenia Gravis (MG)?
MG is an autoimmune disease – your body’s immune system mistakenly attacks the connection between your nerves and muscles.
This causes muscle weakness that gets worse with activity and improves with rest.
Common symptoms:
Droopy eyelids (ptosis) or double vision (diplopia)
Trouble chewing, swallowing, or speaking (slurred or nasal voice)
Weakness in arms, legs, or neck (e.g., trouble holding up your head)
Shortness of breath (if breathing muscles are affected – this is an emergency)
How is MG diagnosed?
Doctors use a combination of:
Blood tests – to look for specific antibodies (AChR, MuSK, LRP4)
Nerve tests (repetitive nerve stimulation or single-fiber EMG) – to check the nerve‑muscle connection
Imaging (CT or MRI of the chest) – to look at the thymus gland
Bedside tests – e.g., the ice‑pack test for droopy eyelids (cold temporarily improves weakness)
The old “Tensilon test” is no longer used due to safety risks.
What treatments are available?
Treatment aims for “minimal symptom expression” – meaning you feel almost normal most of the time.
Medication What it does Important notes
Pyridostigmine (Mestinon) Improves muscle strength within 30‑60 minutes Take as prescribed; side effects (cramps, diarrhea) can often be managed
Prednisolone (steroid) Reduces immune attack – takes weeks to work Now usually taken daily.
You will get a Steroid Alert Card.
Requires bone and stomach protection
Azathioprine, Mycophenolate, Methotrexate Long‑term immune suppression (steroid‑sparing) Azathioprine is safe in pregnancy; mycophenolate and methotrexate are not – discuss family planning
Rituximab Powerful immune therapy – works within weeks
Now recommended early (within 1 year) for generalized MG, especially for MuSK‑MG
Newer targeted therapies (eculizumab, zilucoplan, efgartigimod, rozanolixizumab) For severe or refractory MG
Only under specialist care – require vaccinations (e.g., against meningitis)
Thymectomy (surgery to remove the thymus gland)
Strongly recommended for AChR‑antibody‑positive patients under 50 years old
Should be considered for ages 50–65
Ideally performed within 2 years of diagnosis
Minimally invasive surgery (VATS/robotic) is now standard
What is a myasthenic crisis? (Emergency!)
A crisis is when weakness affects your breathing muscles – this is life‑threatening.
WARNING SIGNS – seek help immediately:
Sudden shortness of breath or trouble taking a deep breath
Can’t count to 25 in one breath
Severe difficulty swallowing or managing saliva
“Neck drop” – head falls forward from weakness
Slurred speech that gets worse
Do NOT rely on a finger oxygen monitor – it can be normal even when breathing muscles are failing.
Triggers to avoid:
Infections, surgery, heat, stress, certain medications (e.g., magnesium, some antibiotics).
Always tell any doctor you have MG before they prescribe new drugs.
Can I fast ?
For many stable patients, yes – but only with your doctor’s approval and if you meet low‑risk criteria.
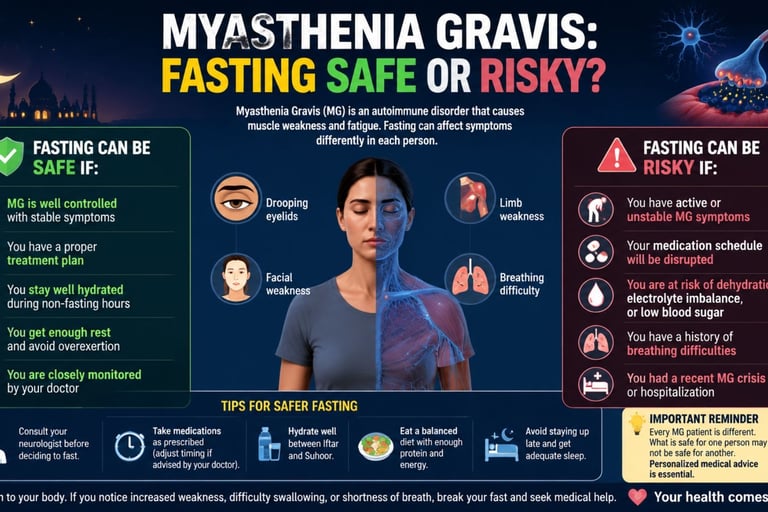
✅ Likely safe to fast if:
Your MG is mild (ocular or mild generalized – MGFA class IIb or lower)
You have been stable for at least 6 months (no recent crises)
You take pyridostigmine ≤240 mg/day and ≤3 doses/day
You are on low‑dose prednisolone (≤5 mg/day) or none
You have no swallowing or breathing problems
Your neurologist agrees
❌ Do NOT fast if:
You have moderate or severe generalized MG (MGFA class III or higher)
You need pyridostigmine more than 3 times daily
You are on high‑dose steroids (>7.5 mg/day) or multiple immunosuppressants
You have had a crisis in the past 6 months
You have difficulty swallowing or breathing
Practical tips if you fast:
Never stop your medications – adjust timing (take at pre‑dawn meal and at sunset meal)
Ask about extended‑release pyridostigmine to last longer
Drink plenty of water between sunset and dawn
Break your fast immediately if you feel weaker, have trouble breathing or swallowing, or get double vision
Carry an emergency card with your diagnosis, medications, and doctor’s phone number
Religious exemption: Islam exempts people with chronic illness from fasting if it would harm their health.
Discuss this with your religious advisor – your health comes first.
What about pregnancy and breastfeeding?
Safe medications: Pyridostigmine, prednisolone, azathioprine, ciclosporin
Avoid (teratogenic): Mycophenolate mofetil, methotrexate (stop at least 6 weeks before trying to conceive)
Newer biologics (FcRn blockers, complement inhibitors) – insufficient safety data; discuss with your specialist
Baby’s health: About 10% of babies have temporary weakness at birth – deliver in a hospital with neonatal support
Fatigue – what helps?
Fatigue is very common in MG (up to 80% of patients).
Important: Fatigue alone is not a sign that your MG is worsening – do not increase your steroids or other MG drugs for fatigue.
Strategies that work:
Pacing – break tasks into small chunks, rest between
Low‑impact exercise – walking, swimming, yoga (avoid overheating)
Respiratory muscle training – especially before thymectomy surgery
Good sleep hygiene and stress management
When should I see a specialist (or be referred)?
Your neurologist should refer you to an MG specialist centre if:
You need repeated hospital admissions or IVIg/plasma exchange
You have a myasthenic crisis (especially if it doesn’t improve quickly)
You are still symptomatic after 3 months on >30 mg/day prednisolone
You cannot reduce prednisolone below 7 mg/day despite other drugs
You need targeted therapies (FcRn blockers, complement inhibitors)
You have MuSK‑antibody MG or are seronegative
You are planning pregnancy or are pregnant with generalized MG
Quick summary table
Goal of treatment Minimal symptom expression (MG‑ADL 0–1) – feel almost normal
First‑line symptomatic Pyridostigmine (Mestinon)
First‑line immune therapy Daily prednisolone + steroid‑sparing agent (azathioprine usually)
Early thymectomy For AChR‑positive patients <50 years (within 2 years of diagnosis)
Rituximab Use early (within 1 year) for generalized MG, especially MuSK+
Fasting Allowed only for stable, mild MG with doctor’s approval
Emergency signs Shortness of breath, can’t count to 25, neck drop, severe swallowing trouble
Pregnancy Avoid mycophenolate and methotrexate; azathioprine is safe
Fatigue Do not escalate MG drugs – use pacing and low‑impact exercise
If I have trouble breathing, swallowing, or my neck gets very weak – I will go to the nearest emergency department and tell them I have Myasthenia Gravis.
myathenia gravis and fasting
The decision to fast for patients with Myasthenia Gravis (MG) is a complex medical choice that depends on the type of MG, disease severity, and medication requirements.
While many patients tolerate fasting well, those with more severe forms of the disease face significant risks of symptom exacerbation.
Clinical Outcomes and Statistics
A landmark study investigating Ramadan fasting (abstaining from all food and drink from dawn to sunset) among MG patients reported the following outcomes:
80.5% of patients remained stable throughout the fasting period.
15% experienced a worsening of symptoms, though 94.1% of these individuals returned to their baseline status after the fast concluded.
4.4% reported an improvement in their clinical condition.
While no patients in the study developed a full myasthenic crisis, some experienced severe weakness in the limb and axial muscles.
Risk Stratification Guidelines
Current clinical guidelines categorize MG patients based on their risk level during prolonged fasts (typically 16–19 hours):
Very High Risk (Must Not Fast): Patients with generalized MG who require regular pyridostigmine (Mestinon) more than 3 times per day, or those with conditions predisposing them to respiratory or bulbar complications.
High Risk (Should Not Fast): Patients on pyridostigmine 3 times daily or less, as the long gaps between doses may lead to a breakthrough of symptoms.
Low to Moderate Risk: Patients with purely ocular MG or those not requiring pyridostigmine may attempt to fast under medical supervision.
Predictors of Symptom Worsening
Certain factors increase the likelihood that a patient's symptoms will deteriorate during a fast:
Having the generalized type of MG rather than purely ocular.
A pre-fasting disease severity of MGFA Class IIIa or IIIb.
Requiring daily pyridostigmine doses of more than 240 mg.
The use of multiple immunosuppressants to maintain disease control.
Metabolic and Personal Impacts
Fasting introduces specific physiological challenges that can interact with myasthenic pathology:
Fatigue and Exhaustion: Fasting-induced fatigue can compound existing myasthenic exhaustion, potentially leading to low blood pressure, low blood sugar, and in some cases, a breathing crisis.
Diurnal Variation: Many MG patients feel stronger in the morning after rest, which can make the early hours of a fast more manageable.
Autophagy and Intermittent Fasting: Some patients theorize that autophagy (the body consuming damaged cells for energy during a fast) may reduce symptoms, though clinical evidence for this is currently lacking. Some report success with intermittent fasting (e.g., a 4-hour eating window), noting it helps with weight loss and reduces fatigue.
Safety and Management Recommendations
Hydration: Maintaining hydration is essential; models of intermittent fasting that allow water are generally safer than total abstinence from liquids.
Medication Adjustment: Patients should work with their neurologist weeks or months before starting a fast to ensure medication timing (such as taking doses at Sehri and Iftar) is compatible with fasting hours.
When to Stop: Patients must be prepared to break the fast immediately if they experience worsening weakness, difficulty breathing, or severe dizziness.
Religious Exemption: It is widely recognized that Islam provides a full exemption from fasting for individuals with chronic illnesses, such as MG, that could be worsened by the practice.
faqs Myasthenia Gravis (MG) – Frequently Asked Questions
1. Diagnosis and General Information
Q1: What is Myasthenia Gravis (MG)?
MG is an autoimmune disease where your immune system attacks the connection between nerves and muscles.
This causes muscle weakness that gets worse with activity and improves with rest.
Q2: What are the first symptoms I might notice?
Most common: droopy eyelids (one or both), double vision, trouble chewing or swallowing, slurred or nasal-sounding speech, and weakness in arms, legs, or neck (e.g., head feels heavy).
Q3: How do doctors diagnose MG?
They use a combination of:
Blood tests for antibodies (AChR, MuSK, LRP4)
Nerve tests (repetitive nerve stimulation or single-fiber EMG)
Chest CT or MRI to check the thymus gland
Bedside tests like the ice‑pack test (cold temporarily improves droopy eyelids)
Q4: Is there a cure for MG?
Not yet, but treatment is very effective. Most people achieve “minimal symptom expression” – meaning they feel almost normal most of the time.
2. Medications and Treatment
Q5: What is the first medication I will take?
Pyridostigmine (Mestinon) – it improves muscle strength within 30–60 minutes. It is not a cure, but it helps with symptoms.
Q6: Do I need steroids?
Most people with moderate to severe MG need prednisolone (a steroid).
The 2025 guidelines recommend taking it daily (not every other day).
Your doctor will start you at a low dose and increase slowly.
You will receive a Steroid Alert Card and need bone and stomach protection.
Q7: What are steroid‑sparing drugs?
These are other immune‑suppressing drugs that allow you to lower your steroid dose.
Examples: azathioprine, mycophenolate, methotrexate.
They take months to work but are very helpful long‑term.
Q8: What is rituximab?
A powerful immune therapy given as an infusion.
The 2025 guidelines recommend using it early (within 1 year of diagnosis) for generalized MG, especially if you have MuSK antibodies.
Q9: What are the newer “targeted” drugs?
These are for people who do not respond to standard treatments:
Complement inhibitors (eculizumab, zilucoplan) – block part of the immune attack. Require meningitis vaccination.
FcRn blockers (efgartigimod, rozanolixizumab) – rapidly reduce harmful antibodies.
They are given only by specialists.
3. Thymectomy (Surgery)
Q10: Will I need surgery to remove my thymus gland?
It depends on your antibody type and age:
If you have AChR antibodies and are under 50 – strongly recommended.
If you are between 50 and 65 – discuss with your surgeon.
If you have MuSK antibodies – surgery is not recommended (unless you have a thymoma tumor).
If you have a thymoma (tumor) – surgery is mandatory.
Q11: When should surgery be done?
Ideally within 2 years of diagnosis – earlier is better.
The surgery is now usually done with minimally invasive techniques (small cuts, faster recovery).
4. Emergency and Crisis
Q12: What is a myasthenic crisis?
A life‑threatening condition where breathing muscles become too weak.
This is a medical emergency.
Q13: What warning signs should I never ignore?
Sudden shortness of breath or trouble taking a deep breath
Cannot count to 25 in one breath
Severe difficulty swallowing or managing saliva
“Neck drop” – your head falls forward
Slurred speech that gets rapidly worse
Do not rely on a finger oxygen monitor – it can be normal even when your breathing is failing. Go straight to the emergency department.
Q14: What triggers a crisis?
Infections, surgery, heat, stress, and certain medications (e.g., magnesium, some antibiotics, high-dose steroids started too quickly). Always tell any doctor you have MG before they prescribe new drugs.
5. Fasting (e.g., Ramadan)
Q15: Can I fast if I have MG?
Maybe – but only if your MG is mild and stable, and your neurologist agrees.
Studies show that about 80% of stable patients can fast safely.
Q16: What makes me a “low‑risk” patient for fasting?
Mild MG (ocular or only mild generalized weakness)
Stable for at least 6 months (no crises or hospital admissions)
Take pyridostigmine ≤240 mg/day and ≤3 doses/day
Low‑dose prednisolone (≤5 mg/day) or none
No swallowing or breathing problems
Q17: When should I NOT fast?
Moderate or severe generalized MG
Need pyridostigmine more than 3 times daily
High‑dose steroids (>7.5 mg/day) or multiple immune drugs
Had a crisis in the past 6 months
Difficulty swallowing or breathing
Q18: If I fast, how should I take my medications?
Never stop your medications. Adjust timing with your doctor.
Take pyridostigmine at the pre‑dawn meal (suhoor) and at sunset (iftar). Ask about extended‑release versions.
Take prednisolone with food at iftar to protect your stomach.
Drink plenty of water between sunset and dawn.
Q19: When should I break my fast immediately?
If you feel weaker, have trouble breathing or swallowing, get double vision, or feel very dizzy – break the fast and contact your doctor.
Q20: Is there a religious exemption?
Yes – Islam exempts people with chronic illness from fasting if it would harm their health. Your health comes first.
6. Pregnancy and Family Planning
Q21: Can I get pregnant if I have MG?
Yes. Most women with well‑controlled MG have normal pregnancies. However, you must plan with your neurologist and obstetrician.
Q22: Which MG medications are safe during pregnancy?
Safe: Pyridostigmine, prednisolone, azathioprine, ciclosporin
NOT safe (teratogenic): Mycophenolate mofetil, methotrexate (stop at least 6 weeks before trying to conceive)
Newer drugs (FcRn blockers, complement inhibitors) – not enough data; discuss with your specialist
Q23: Will my baby be affected?
About 10% of babies have transient neonatal myasthenia (temporary weakness at birth). They recover completely with treatment. Deliver in a hospital with neonatal support.
Q24: Can I breastfeed?
Yes – pyridostigmine, prednisolone, and azathioprine are considered safe during breastfeeding.
7. Lifestyle, Exercise, and Fatigue
Q25: I feel tired all the time – is my MG getting worse?
Fatigue affects up to 80% of people with MG. Fatigue alone is not a sign of worsening MG. Do not increase your steroids or other MG drugs just for fatigue – talk to your doctor first.
Q26: What helps with fatigue?
Pacing – break activities into small chunks, rest in between
Low‑impact exercise – walking, swimming, yoga (avoid overheating)
Good sleep and stress management
Respiratory muscle training – especially before thymectomy
Q27: Can I exercise?
Yes – gentle, regular exercise is beneficial. Avoid exercise when you are very hot or already tired. Stop if weakness worsens significantly.
Q28: What should I avoid?
Overheating (hot baths, saunas, hot weather)
Skipping meals or becoming dehydrated
Certain medications (always check with your pharmacist or doctor)
Stress and lack of sleep
8. When to See a Specialist
Q29: When should my neurologist refer me to an MG specialist centre?
Repeated hospital admissions or need for IVIg/plasma exchange
A myasthenic crisis (especially if slow to recover)
Still symptomatic after 3 months on >30 mg/day prednisolone
Cannot reduce prednisolone below 7 mg/day despite other drugs
Need for targeted therapies (FcRn blockers, complement inhibitors)
MuSK‑antibody MG or seronegative MG
Planning pregnancy or pregnant with generalized MG
9. Quick Reference – Emergency Card
Cut out and carry this card in your wallet:
⚠️ EMERGENCY SIGNS (go to ER immediately):
- Shortness of breath / can't count to 25 in one breath
- Severe trouble swallowing or managing spit
- Neck drop (head falls forward)
- Slurred speech that worsens
DO NOT give me: magnesium, aminoglycoside antibiotics, or botulinum toxin.
This FAQ is based on the 2025 Association of British Neurologists (ABN) guidelines for myasthenia gravis.
Always follow the specific advice of your own medical team.
==================================================================================================================================================================================
🌙🧠Myasthenia Gravis: Fasting Safe or Risky?
https://www.h-k-e-m.com/myasthenia-gravisfasting-safe-or-risky
🌙🧠 Myasthenia Gravis: Fasting – Safe or Risky?
A Quick Summary (Based on 2025 Guidelines)
Fasting (e.g., during Ramadan) can be safe for some people with MG, but only if they are carefully selected and under medical supervision. For others, it is risky and not recommended.
✅ When is fasting likely safe?
All of these must apply:
Mild disease – ocular MG or mild generalized MG (MGFA class IIb or lower)
Stable for ≥6 months – no crises, no hospital admissions
Low medication burden:
Pyridostigmine ≤240 mg/day and ≤3 doses/day
Prednisolone ≤5 mg/day (or none)
No swallowing or breathing problems
Your neurologist approves
About 80% of stable, mild patients fast safely based on clinical studies.
❌ When is fasting risky (should be avoided)?
Moderate to severe generalized MG (MGFA class III or higher)
Unstable disease – recent crisis (<6 months) or frequent relapses
High medication needs:
Pyridostigmine >240 mg/day or ≥4 doses/day
Prednisolone >7.5 mg/day
Multiple immunosuppressants
Dysphagia (swallowing difficulty) or respiratory weakness
No medical supervision or doctor’s approval
⚠️ Critical rules if you fast:
Never stop your MG medications – adjust timing (pre-dawn and sunset meals).
Break the fast immediately if you develop:
Shortness of breath or cannot count to 25 in one breath
Severe difficulty swallowing or slurred speech
Sudden worsening of weakness or “neck drop”
Double vision or severe dizziness
Stay hydrated between fast-breaking hours.
Keep an emergency plan – doctor’s number, medical alert card.
🩺 Bottom line
Fasting is not a treatment for MG. It does not fix your immune system.
For stable, mild MG under medical guidance, fasting may be safe.
For anyone with moderate/severe, unstable, or high‑medication MG, fasting is risky and not advised.
Always ask your neurologist before fasting – your safety comes first.
Keywords:
myasthenia gravis fasting, fasting and myasthenia gravis, myasthenia gravis symptoms, muscle weakness and fasting, autoimmune disease fasting, fasting safety myasthenia gravis, MG medication during fasting, neuromuscular disease fasting, Ramadan and myasthenia gravis, fatigue during fasting, fasting health risks, hydration and myasthenia gravis, intermittent fasting autoimmune disease, myasthenia gravis management, fasting precautions
Hashtags:
#MyastheniaGravis #Fasting #AutoimmuneDisease #Neurology #MuscleWeakness #RamadanHealth #IntermittentFasting #ChronicIllness #HealthAwareness #MedicalEducation #HealthyFasting #NeuromuscularDisease #PatientEducation #Wellness #Healthcare
=================================================================================================================================================================================================================================================================================================================================================================================================================================
⚖️ Why does the world hate Israel, not Jews?
1. The Core Distinction: A State vs. a People
Israel is a nation-state with a government, an army, and specific policies (e.g., occupation of the West Bank, blockade of Gaza, settlement expansion). Criticizing these actions is a political stance, not a racial or religious one.
Jews are a diverse ethno-religious group with a 3,000+ year history, living all over the world. Hating Jews means targeting individuals for their identity, not their government’s actions.
Thus, from this perspective:
“I can oppose Israeli settlements without opposing Shabbat dinner.”
2. Why Israel Draws Unique Global Scrutiny (The “World Hates Israel” perception)
Many pro-Israel advocates argue that the world does treat Israel unfairly compared to other nations. For example:
Disproportionate UN resolutions: Since 2015, the UN General Assembly has passed more resolutions condemning Israel than all other countries combined (including Syria, North Korea, Iran).
Boycott movements (BDS): No other country faces a coordinated global movement to isolate it economically and culturally.
Media focus: A military clash in Gaza often gets more front-page coverage than far deadlier conflicts (e.g., in Yemen, Ethiopia, or Myanmar).
Critics of Israel say this focus is because of its ongoing occupation and its unique status as a Western-backed democracy in the Middle East. Supporters of Israel say it’s evidence of a double standard—often motivated by anti-Jewish bias disguised as anti-Zionism.
3. Why People Say “It’s Not About Jews”
Many who oppose Israel’s actions go out of their way to clarify they are not antisemitic:
Many Jews oppose Israel’s policies – groups like Jewish Voice for Peace or Neturei Karta actively protest the Israeli government.
Criticism of a country is normal – people criticize China’s Uyghur policy, Russia’s invasion of Ukraine, or America’s drone strikes without being called “anti-Chinese” or “anti-American.”
The issue is occupation and military force – the core complaint is about land, borders, checkpoints, home demolitions, and civilian casualties, not about Judaism.
From this view, conflating anti-Zionism with antisemitism is a tactic to silence legitimate criticism.
4. Why Many Jews See Anti-Zionism as Antisemitism (The Overlap)
While the distinction sounds clean in theory, in practice the line often vanishes:
Classic antisemitic tropes reappear: Critics of Israel sometimes describe it as controlling the media, the banks, or the US Congress – the same conspiracies used against Jews historically.
Denying Jewish self-determination: Opponents of a Jewish state (not just its policies) argue that Jews should not have a nation anywhere. Many Jews hear that as: “You can live as a tolerated minority elsewhere, but you cannot have sovereignty like every other people.”
Violence spills over: After an Israeli military operation, synagogues in Europe or the US are often vandalized, and Jews are attacked. The attacker rarely distinguishes between “Israeli policy” and “Jewish person.”
Thus, many Jews conclude: “When you say ‘Zionism = racism’ or chant ‘From the river to the sea,’ you are calling for the end of the only Jewish state. That makes Jews uniquely vulnerable worldwide.”
5. So Who Actually “Hates Israel” and Who “Hates Jews”?
GroupStance on IsraelStance on JewsMainstream critics (e.g., Amnesty, HRW, many UN members)Condemn specific policies (occupation, settlements, military tactics)No hatred of Jews; many are Jewish themselvesAnti-Zionists (e.g., some Palestinian activists)Oppose the existence of a Jewish stateOften say they don’t hate Jews, only political Zionism; but their rhetoric can blur linesAntisemites (e.g., neo-Nazis, white supremacists, Islamist extremists)May also hate IsraelIntrinsically hate Jews, regardless of IsraelPro-Israel advocatesSupport Israel’s right to exist and defend itselfDefend Jewish rights globally
The Bottom Line
The world does not “hate” either in a monolithic way. Polls show many people have nuanced views: they may dislike Israel’s government while having positive views of Jewish people.
The perception of “hating Israel, not Jews” comes from those who believe that intense, single-minded focus on Israeli misdeeds while ignoring worse abuses elsewhere is a form of antisemitism (the “new antisemitism”).
The counter-perception is that Israel uses antisemitism accusations to shield itself from legitimate criticism of its military occupation and human rights record.
Ultimately, your question touches on an unresolved debate. Are critics of Israel holding it to a higher standard because of its Jewish identity (antisemitic double standard) or because it is a Western-backed democracy engaged in a decades-long military occupation (political and moral critique)? There is no single answer—only clashing frameworks.
If you'd like, I can walk you through the history of Zionism and the roots of this split, or discuss how to spot when anti-Zionism crosses into antisemitism.




Get in touch
Address
Cairo Al Rehab
Contacts
+20 109 405 2056
hassanalwarraqi@h-k-e-m.com