
Health is a crown on the heads of the healthy that only the sick can see.


🧠👂 Metabolic Shift & ⟴ Vestibular Balance : BPPV & Fasting 🌙
Clinical guide exploring how metabolic changes during fasting may influence vestibular balance and symptoms of Benign Paroxysmal Positional Vertigo (BPPV)
FASTINGNERVOUS SYSTEM EAR NOSE AND THROATS OTOLARYNGOLOGY
Dr Hassav Al Warraqi
3/7/202612 min read

🧠👂 Metabolic Shift & ⟴ Vestibular Balance : BPPV & Fasting 🌙
Clinical guide exploring how metabolic changes during fasting may influence vestibular balance and symptoms of Benign Paroxysmal Positional Vertigo (BPPV)
Bottom line: BPPV is highly treatable.
Most cases resolve within one or two clinic visits using simple repositioning maneuvers.
However, dizziness has many causes — from benign inner ear crystals to strokes.
Accurate diagnosis is the critical first step.
This guide explains both: how BPPV is identified and managed, and how to distinguish it from other causes of dizziness.
Understanding the Condition
What Is BPPV?
Benign Paroxysmal Positional Vertigo (BPPV) is the most common vestibular disorder — a condition of the inner ear that causes brief, intense episodes of spinning dizziness triggered by specific changes in head position.
The name describes it precisely: benign (not dangerous), paroxysmal (sudden and brief), positional (triggered by head position), vertigo (a false sensation of movement).
BPPV occurs when tiny calcium carbonate crystals called otoconia dislodge from their normal location in the utricle — a gravity-sensing chamber in the inner ear — and migrate into one of the three semicircular canals.
These crystals interfere with normal fluid movement inside the canals, sending erroneous motion signals to the brain every time the head moves into a certain position.
How it works
🔬 The Otoconia Mechanism
Normally, otoconia crystals sit atop hair cells in the utricle and help detect linear acceleration and gravity.
When they break free and enter a semicircular canal, they create fluid currents that shouldn't be there — triggering a sensation of spinning that lasts seconds to a minute.
Key symptoms
😵 What Patients Experience
A sudden intense spinning sensation provoked by: rolling over in bed, tilting the head back, bending forward, or sitting up quickly.
Episodes last under a minute and are often accompanied by nausea.
Between episodes, patients feel completely normal.
◆
Clinical Diagnosis
How BPPV Is Diagnosed
Diagnosis relies on a thorough clinical history and specific physical examination maneuvers designed to provoke vertigo and observe characteristic eye movements — nystagmus (involuntary rhythmic eye oscillations).
These maneuvers are the gold standard because BPPV leaves no trace on standard imaging or blood tests.
Dix-Hallpike Maneuver — Gold Standard for Posterior Canal BPPV
The most widely recognized diagnostic test.
The clinician rapidly moves the patient from sitting to lying supine with their head rotated 45 degrees to one side and extended approximately 20 degrees below horizontal.
The clinician watches closely for nystagmus — its direction, latency, duration, and fatigability all help identify the specific canal affected.
Upbeating torsional nystagmus with a brief latency and duration under 60 seconds confirms posterior canal BPPV.
The test is repeated on the opposite side to determine which ear is affected.
Supine Head Roll Test — For Horizontal Canal BPPV
When the Dix-Hallpike is negative but BPPV is still suspected, the Supine Head Roll Test (Roll Maneuver) is used to assess the horizontal canal.
The patient lies flat on their back, and the examiner rapidly rotates the head 90 degrees to each side.
The side producing stronger, more intense nystagmus or vertigo typically identifies the affected ear.
Horizontal nystagmus that beats toward the ground (geotropic) suggests canalith particles; nystagmus beating away from the ground (apogeotropic) may indicate a cupulolithiasis variant.
🔍 Why Nystagmus Matters
The precise pattern of nystagmus observed during diagnostic maneuvers is the clinician's map to the exact canal and side involved.
Posterior canal BPPV produces upbeating-torsional nystagmus.
Horizontal canal BPPV produces purely horizontal nystagmus.
Anterior canal BPPV (rare) produces downbeating nystagmus.
Getting the canal right is essential — treating the wrong canal with the wrong maneuver will not resolve symptoms and may worsen them.
◆
Particle Repositioning Maneuvers
Treating BPPV: Moving the Crystals Back
The primary treatment for BPPV is particle repositioning maneuvers (PRMs) — carefully sequenced head and body movements that use gravity to guide displaced otoconia out of the semicircular canal and back into the utricle where they can no longer cause problems.
These are among the most effective non-pharmacological treatments in clinical medicine, with resolution rates exceeding 80% after a single session for posterior canal BPPV.
For Posterior Canal BPPV (Most Common)
Epley Maneuver — First-Line Treatment
The most widely used and evidence-supported treatment for posterior canal BPPV.
The maneuver involves a sequence of four head and body positions — beginning with the Dix-Hallpike position on the affected side, then rotating the head 90 degrees to the opposite side, then rolling the entire body to the side while keeping the head turned, and finally sitting up.
Each position is held for 30 seconds or until nystagmus resolves.
Patients can be taught a modified self-treatment version (the home Epley) to manage recurrences independently.
Success rates are typically 70–90% after one or two treatments.
Semont Maneuver — The Liberatory Maneuver
Also known as the liberatory maneuver, the Semont Maneuver involves rapidly moving the patient from sitting to lying on the affected side, then swinging them in a single rapid arc to the opposite side.
It is particularly useful when the Epley maneuver is not feasible — for example in patients with limited neck mobility — or when the Epley has been unsuccessful.
Evidence supports comparable efficacy to the Epley maneuver for posterior canal BPPV.
Brandt-Daroff Exercises — Home-Based Option
These exercises involve rapidly moving from sitting to side-lying position on alternating sides, repeated multiple times in a session.
They are less effective than the Epley or Semont maneuvers when compared directly, and symptoms may take days to weeks to resolve rather than a single session.
However, Brandt-Daroff exercises are a reasonable home-based option for patients who cannot access in-person treatment or as a supplement between clinic visits.
They are thought to work through habituation rather than physical repositioning.
For Horizontal Canal BPPV
Lempert Maneuver (Barbecue Roll)
The Lempert maneuver guides otoconia out of the horizontal canal through a series of sequential 90-degree head rotations while the patient lies flat — effectively rolling the patient through 270 degrees in incremental steps.
The "Barbecue Roll" nickname captures the technique well.
It is the standard first-line treatment for geotropic horizontal canal BPPV and is highly effective when performed correctly.
Gufoni Maneuver
The Gufoni maneuver involves rapidly moving the patient from sitting to a side-lying position, pausing, then quickly turning the head 45 degrees in a specific direction.
It is particularly well-suited for ageotropic horizontal canal BPPV (the cupulolithiasis variant, where nystagmus beats away from the ground).
The Gufoni maneuver is often preferred by clinicians for this subtype due to its simplicity and strong efficacy data.
📊 Treatment Effectiveness at a Glance
Summary of resolution rates and key clinical characteristics for each maneuver:
80–90%
Epley — single session resolution rate (posterior canal)
~80%
Semont — comparable to Epley; preferred for limited neck ROM
Weeks
Brandt-Daroff — slower resolution; works via habituation
Barbecue
Lempert — first-line for horizontal canal geotropic BPPV
◆
Differential Diagnosis
General Causes of Dizziness: Beyond BPPV
Dizziness is one of the most common complaints in clinical medicine and one of the most diagnostically challenging.
The term encompasses several distinct sensations — vertigo (spinning), lightheadedness (faintness), disequilibrium (unsteadiness), and presyncope (near-fainting) — each pointing toward a different underlying mechanism.
Causes span three broad categories.
🦻 Vestibular Causes (Inner Ear)
BPPV
— The most common cause of vertigo. Discrete positional episodes lasting under one minute, resolved by repositioning maneuvers.
Menière's Disease
— Episodes of severe rotational vertigo lasting 20 minutes to several hours, accompanied by fluctuating hearing loss, tinnitus (ringing), and aural fullness.
Caused by abnormal endolymphatic pressure.
Vestibular Neuritis / Labyrinthitis
— Sudden severe vertigo with nausea and imbalance lasting days, caused by viral inflammation of the vestibular nerve or inner ear.
Labyrinthitis also involves hearing loss.
Vestibular Migraine / Migrainous Vertigo
— Episodic vertigo associated with migraine, sometimes without headache.
Duration varies from minutes to days; a frequently underdiagnosed condition.
❤️ Non-Vestibular Causes
💉
Cardiovascular
Orthostatic hypotension, arrhythmias, and heart failure reduce cerebral perfusion, causing lightheadedness on standing or exertion.
🩸
Metabolic
Dehydration, hypoglycemia, and anemia all reduce oxygen and glucose delivery to the brain — producing faintness, weakness, and dizziness.
💊
Medications
Blood pressure drugs, sedatives, antidepressants, anticonvulsants, and pain relievers commonly list dizziness as a side effect.
🧠
Anxiety / Panic
Chronic dizziness and unsteadiness can be a primary manifestation of anxiety and panic disorder — sometimes called PPPD (persistent postural-perceptual dizziness).
🌡️
Dehydration
Insufficient fluid intake reduces blood volume directly, causing lightheadedness — often confused with vestibular vertigo.
🔬
Anemia
Low red blood cell count reduces brain oxygenation, particularly on exertion — producing fatigue and lightheadedness distinct from spinning vertigo.
🧠 Central Causes (Brain)
⚠️ When Dizziness Is a Red Flag
Stroke / TIA
— Sudden onset dizziness with neurological signs (weakness, facial droop, speech changes, double vision, severe headache) is a medical emergency.
HINTS exam (Head Impulse, Nystagmus, Test of Skew) can differentiate central from peripheral vertigo at the bedside.
Brain Tumors
— Tumors of the cerebellum or brainstem produce progressive dizziness, imbalance, and other neurological symptoms without the discrete episodic pattern of BPPV.
Multiple Sclerosis
— MS lesions in the brainstem or cerebellum can cause dizziness and balance problems alongside other neurological features.
Vestibular Migraine
— A central-peripheral overlap condition:
vestibular symptoms driven by brainstem migraine mechanisms, sometimes without headache.
🎯 The HINTS Exam: Bedside Rule-Out for Stroke
In the emergency setting, the HINTS exam (Head Impulse Test + Nystagmus pattern + Test of Skew) has higher sensitivity for posterior fossa stroke than early MRI.
Abnormal head impulse test + direction-changing nystagmus + skew deviation = central cause until proven otherwise. Any clinician evaluating acute continuous dizziness should be familiar with this three-step bedside tool.
The Bottom Line
BPPV & Dizziness: What the Evidence Says
BPPV is one of the most treatable conditions in medicine — a mechanical problem with a mechanical solution.
Most patients with posterior canal BPPV are cured in a single office visit with the Epley maneuver.
The clinical challenge lies in recognizing it accurately, distinguishing it from other causes of dizziness, and knowing when dizziness represents something more serious that requires urgent evaluation.
BPPV Essentials
Displaced otoconia in semicircular canals
Episodes under 60 seconds, positional trigger
Diagnosed with Dix-Hallpike or Roll Test
Treated with Epley or Lempert maneuver
Can self-recur; home Epley for recurrences
Red Flag Symptoms
Dizziness + neurological signs → stroke workup
Continuous dizziness for days → vestibular neuritis
Episodic hearing loss + tinnitus → Menière's
Dizziness only on standing → orthostatic hypotension
New severe headache + dizziness → emergency
When to Seek Help
First episode of severe vertigo
Dizziness lasting more than 24 hours
Any associated neurological symptoms
Falls or significant balance impairment
Dizziness not responding to maneuvers
Medical Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment.
Dizziness has many causes, some of which require urgent evaluation.
Always consult a qualified healthcare professional for assessment and management of vertigo, dizziness, or balance problems.
Benign Paroxysmal Positional Vertigo (BPPV) and Fasting: Exploring the Relationship FAQS
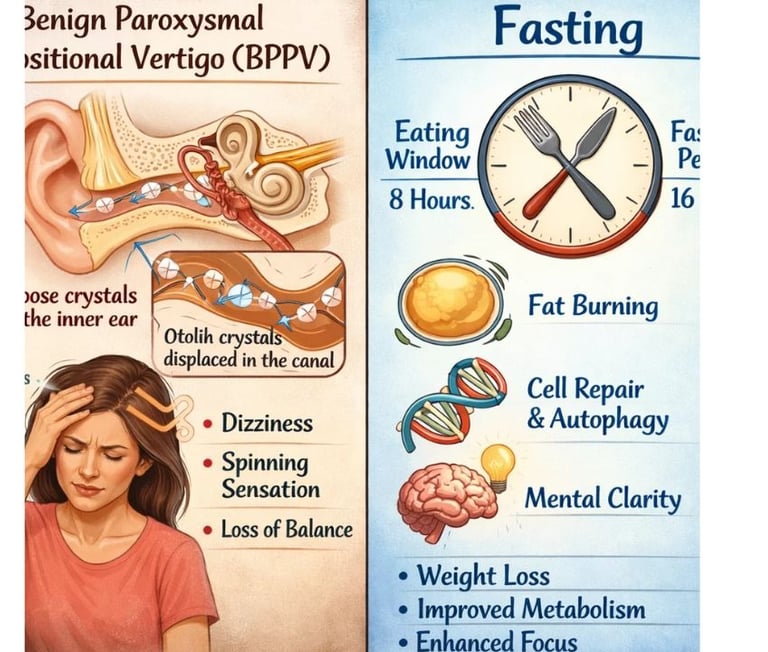
Benign Paroxysmal Positional Vertigo (BPPV) is a common vestibular disorder characterized by brief, intense episodes of vertigo triggered by specific head movements.
While the primary cause of BPPV is the displacement of calcium carbonate crystals (otoconia) within the inner ear, patients often inquire about the role of dietary habits, particularly fasting, in the onset or management of their symptoms.
This report explores the potential physiological links between fasting and BPPV, the impact of metabolic changes, and practical management strategies.
The Physiological Link Between Fasting and BPPV
There is no direct, scientifically established evidence that fasting causes the initial displacement of otoconia that leads to BPPV.
However, fasting induces several physiological changes that can indirectly influence the vestibular system and the perception of vertigo symptoms.
Dehydration and Inner Ear Fluid Balance
Fasting, especially when fluid intake is restricted (as in some religious fasts), can lead to dehydration.
The inner ear relies on a precise balance of fluids—endolymph and perilymph—to function correctly.
•Endolymphatic Homeostasis: Dehydration can alter the concentration of ions (such as sodium and potassium) in the endolymph .
These ionic changes can impair the energy supply to the inner ear and affect the signaling of vestibular nerves, potentially exacerbating the sensation of dizziness or imbalance .
•Otoconia Stability: While not directly proven, some researchers suggest that chronic dehydration or significant electrolyte imbalances might affect the biochemical environment of the utricle, potentially influencing the stability of the otoconia .
Metabolic Changes and Glucose Regulation
Fasting leads to a drop in blood glucose levels and changes in insulin sensitivity.
The inner ear is highly metabolically active and sensitive to glucose fluctuations.
•Energy Supply: Glucose is essential for the production of energy required to maintain the ionic gradients in the inner ear
. Hypoglycemia (low blood sugar) can lead to lightheadedness and faintness, which may be mistaken for or worsen the distress caused by BPPV-related vertigo .
•Insulin Resistance: Some studies have suggested a link between insulin resistance, hyperinsulinemia, and vestibular disorders.
While BPPV is primarily a mechanical issue, underlying metabolic disturbances may slow down the process of vestibular
compensation—the brain's ability to adapt to the faulty signals from the inner ear .
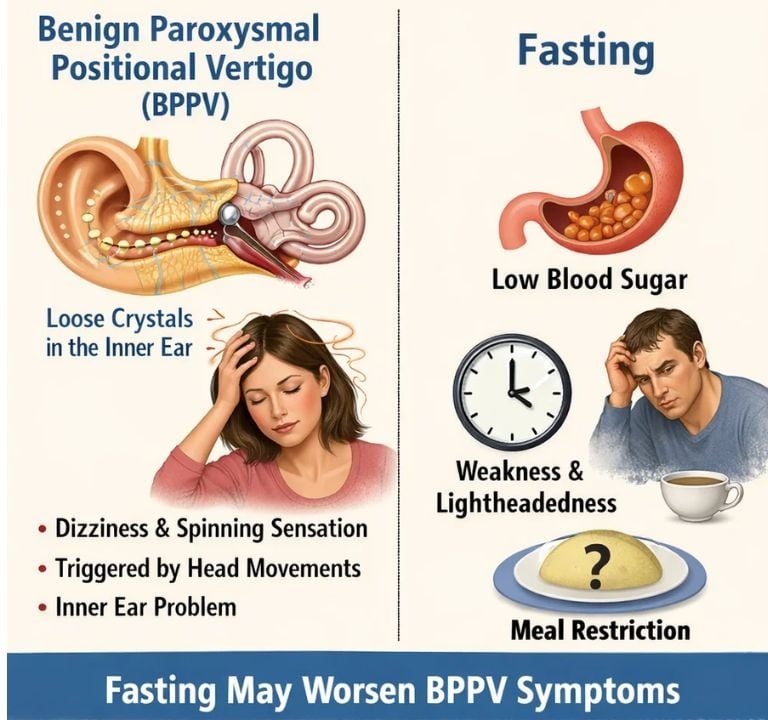
Fasting as a Trigger vs. Exacerbating Factor
It is important to distinguish between fasting as a cause of BPPV and fasting as a factor that makes the symptoms more difficult to manage.
No established evidence that fasting causes otoconia to dislodge.
Symptom Exacerbation
Dehydration and low blood sugar can increase the intensity of dizziness.
Vestibular Compensation
Metabolic stress from fasting may slow the brain's adaptation to vertigo.
Differential Diagnosis
Fasting-induced lightheadedness can be confused with BPPV-related vertigo.
Management Strategies for Fasting with BPPV
For individuals with BPPV who choose to fast, several strategies can help minimize the impact on their vestibular health:
1.Prioritize Hydration: During non-fasting hours, ensure adequate intake of water and electrolytes to maintain inner ear fluid balance .
2.Stable Glucose Levels: When breaking a fast, choose complex carbohydrates and proteins to avoid rapid spikes and subsequent drops in blood sugar .
3.Monitor Symptoms: Be aware that BPPV is specifically triggered by head position changes (e.g., rolling over in bed).
If dizziness is constant or occurs only when standing up, it may be related to orthostatic hypotension or low blood sugar rather than BPPV .
4.Medical Consultation: If BPPV symptoms are active, it is advisable to consult a healthcare professional before starting a prolonged fast, as the combined stress of vertigo and fasting can increase the risk of falls .
Conclusion
While fasting is not a direct cause of BPPV, the physiological changes it induces—particularly dehydration and glucose fluctuations—can significantly impact the vestibular system.
These changes may exacerbate the sensation of vertigo and potentially delay the recovery process.
Maintaining proper hydration and stable nutrition during non-fasting periods is essential for individuals managing BPPV.
Dr Hassan Al Warraqi Clinical Message
The fasting approach attributed to Hassan Al-Warraqi proposes:
fasting 3–4 days per week or daily time-restricted fasting
continuation of all medical treatments
temporary pause during procedures
resumption after approximately two days of recovery
For vestibular conditions such as Benign Paroxysmal Positional Vertigo, fasting may be considered a supportive metabolic strategy, not a replacement for medical care.
Frequently Asked Questions: Benign Paroxysmal Positional Vertigo (BPPV) and Fasting
This document addresses common questions regarding Benign Paroxysmal Positional Vertigo (BPPV) and its potential relationship with fasting.
While BPPV is primarily a mechanical inner ear disorder, certain physiological changes associated with fasting can influence its symptoms or management.
General BPPV Questions
Q1: What is BPPV?
A1: Benign Paroxysmal Positional Vertigo (BPPV) is a common inner ear disorder that causes brief, intense episodes of dizziness or a spinning sensation (vertigo).
These episodes are typically triggered by specific changes in head position, such as looking up, lying down, or turning over in bed .
It occurs when tiny calcium carbonate crystals (otoconia) dislodge from their normal position in the utricle and migrate into one of the semicircular canals of the inner ear .
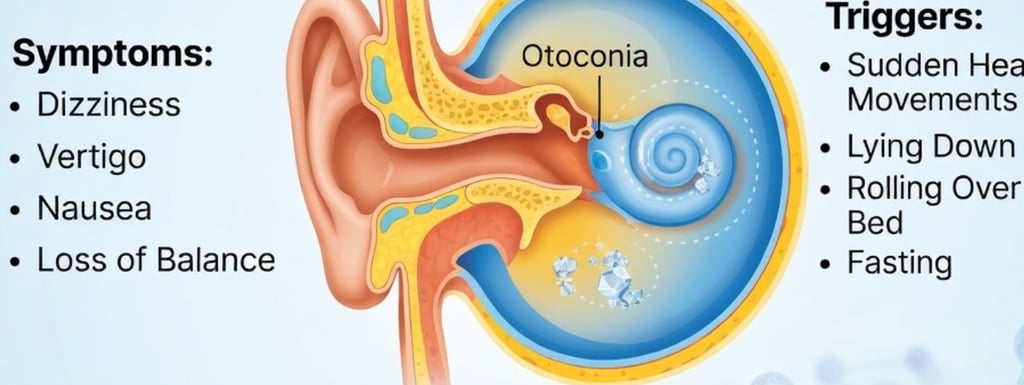
Q2: What are the common symptoms of BPPV?
A2: The primary symptom of BPPV is vertigo, which is a sensation of spinning or that the world is spinning around you.
Other symptoms can include lightheadedness, imbalance, nausea, and occasionally vomiting. These symptoms usually last for less than a minute per episode and are provoked by head movements .
Q3: How is BPPV diagnosed?
A3: BPPV is typically diagnosed through a physical examination, most notably the Dix-Hallpike maneuver for posterior canal BPPV.
This maneuver involves specific head and body movements designed to provoke vertigo and observe characteristic eye movements (nystagmus), which confirms the diagnosis and identifies the affected ear and canal . For horizontal canal BPPV, the Supine Head Roll Test is used .
Q4: How is BPPV treated?
A4: BPPV is primarily treated with particle repositioning maneuvers (PRMs), which are a series of specific head and body movements designed to move the displaced otoconia out of the semicircular canals and back into the utricle.
The most common and effective maneuver for posterior canal BPPV is the Epley maneuver .
Other maneuvers include the Semont maneuver and Brandt-Daroff exercises .
For horizontal canal BPPV, the Lempert (Barbecue Roll) maneuver or Gufoni maneuver may be used .
BPPV and Fasting Questions
Q5: Can fasting cause BPPV?
A5: There is no direct scientific evidence to suggest that fasting directly causes the initial displacement of otoconia,
which is the underlying cause of BPPV .
BPPV is primarily a mechanical problem within the inner ear .
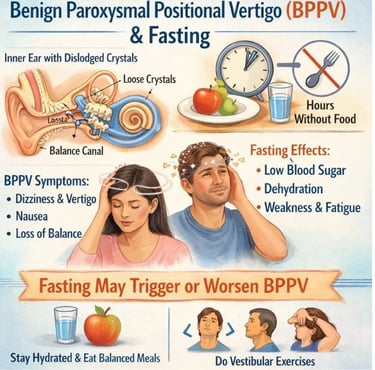
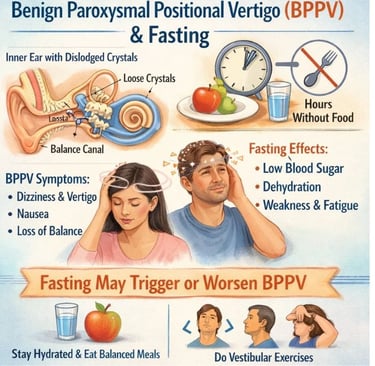
Q6: Can fasting worsen BPPV symptoms or trigger episodes?
A6: While fasting may not directly cause BPPV, the physiological changes associated with it can potentially exacerbate BPPV symptoms or make individuals more susceptible to experiencing dizziness.
Key factors include:
•Dehydration: Insufficient fluid intake during fasting can lead to dehydration, which affects the fluid balance in the inner ear (endolymph and perilymph).
This imbalance can impair the function of the vestibular system and worsen feelings of dizziness or unsteadiness .
•Blood Sugar Fluctuations: Fasting can lead to lower blood sugar levels (hypoglycemia).
The inner ear requires a stable supply of glucose for optimal function.
Low blood sugar can cause lightheadedness, weakness, and a general feeling of faintness, which can be confused with or add to the distress of BPPV-related vertigo .
Q7: Should I avoid fasting if I have BPPV?
A7: If you have BPPV and are considering fasting,
it is highly recommended to consult with your healthcare provider.
They can assess your individual health status, the severity and frequency of your BPPV episodes,
and any other medical conditions you may have. They can provide personalized advice on whether fasting is safe for you and how to manage potential risks .
Q8: What precautions can I take if I fast with BPPV?
A8: If you choose to fast with BPPV, consider the following precautions:
•Stay Hydrated: During non-fasting periods, ensure you drink plenty of fluids, especially water and electrolyte-rich beverages, to prevent dehydration .
•Balanced Nutrition: When you break your fast, consume a balanced diet with complex carbohydrates, proteins, and healthy fats to maintain stable blood sugar levels and provide essential nutrients .
•Monitor Symptoms: Pay close attention to your body.
If you experience increased dizziness, lightheadedness, or any other concerning symptoms, break your fast and seek medical advice.
•Avoid Sudden Movements: Continue to be mindful of head movements that typically trigger your BPPV symptoms.
Q9: Can diet, in general, affect BPPV?
A9: While diet is not a direct cause of BPPV, emerging research suggests a potential link between certain dietary patterns and the progression or recurrence of BPPV.
For instance, some studies indicate associations between BPPV and inadequate carbohydrate intake, high polyunsaturated fatty acid intake, and insufficient fiber .
Maintaining a healthy, balanced diet and addressing any nutritional deficiencies (e.g., Vitamin D) may contribute to overall inner ear health and potentially reduce BPPV recurrence .
===================================================================================================================================================================================
🧠👂 Metabolic Shift & ⟴ Vestibular Balance : BPPV & Fasting 🌙
https://www.h-k-e-m.com/-metabolic-shift-and-vestibular-balance-bppv-and-fasting-
BPPV fasting, fasting and vertigo, vestibular stability fasting, metabolic shift vertigo, BPPV and metabolism
inner ear balance fasting, positional vertigo triggers, dehydration vertigo, vestibular disorders fasting, otolith dysfunction
===================================================================================================================================================================================

Get in touch
Address
Cairo Al Rehab
Contacts
+20 109 405 2056
hassanalwarraqi@h-k-e-m.com