
Health is a crown on the heads of the healthy that only the sick can see.


👁️🌙 Eye Health, Glaucoma & Fasting Protocols · A Scientific Overview
Explore the scientific relationship between glaucoma and fasting. Learn how fasting affects intraocular pressure, optic nerve health, hydration balance, and clinical management strategies for safe fasting in glaucoma patients.
FASTINGEYE DISEASE
Dr Hassan Al Warraqi
3/3/202616 min read
👁️🌙 Eye Health, Glaucoma & Fasting Protocols · A Scientific Overview
Explore the scientific relationship between glaucoma and fasting. Learn how fasting affects intraocular pressure, optic nerve health, hydration balance, and clinical management strategies for safe fasting in glaucoma patients.
Eye Health, Glaucoma & Fasting Protocols | Scientific Clinical Overview
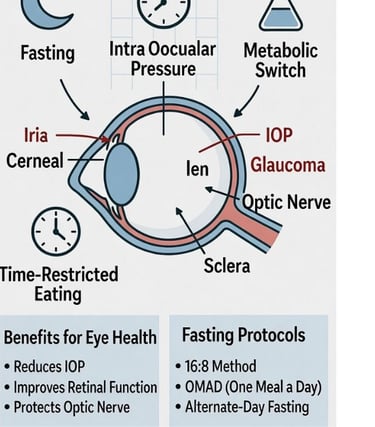
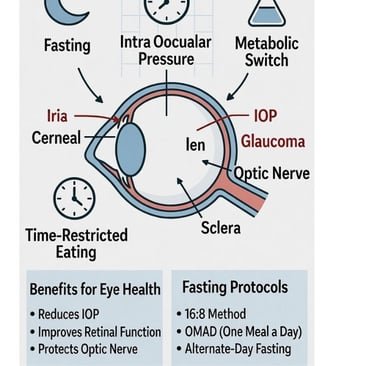
Glaucoma is a chronic optic neuropathy characterized by progressive damage to the optic nerve, most commonly associated with elevated intraocular pressure.
As fasting practices—particularly intermittent fasting and Ramadan fasting—become increasingly common worldwide, clinicians and patients alike are asking important questions about their potential impact on ocular physiology.
This scientific overview examines the relationship between fasting and glaucoma, focusing on intraocular pressure dynamics, hydration status, vascular perfusion, metabolic changes, and evidence-based clinical recommendations for safe practice.
While fasting may offer systemic metabolic benefits, glaucoma management remains centered on consistent pressure control and regular ophthalmic monitoring.
A comprehensive, evidence-based guide covering IOP dynamics, rehydration risks,
Normal Tension Glaucoma, Ramadan medication guidance, and neuroprotective science.
↓↑
IOP changes with dehydration and rehydration
40%
Vision lost before symptoms noticed
NTG
Vascular risk may exceed IOP risk
✓
Drops do not break the fast
Bottom Line, Upfront
Most people with glaucoma can fast safely — but only with careful planning and uninterrupted medication.
Eye drops do NOT break the fast according to the overwhelming consensus of Islamic scholars and medical associations. Stopping them, even briefly, risks permanent and irreversible vision loss.
That is the central clinical message of everything that follows.
◆ UNDERSTANDING THE DISEASE
Two Types of Glaucoma — One Goal
Glaucoma is not a single disease but a family of conditions united by progressive optic nerve damage.
The two dominant forms differ critically in their mechanism and urgency, but share the same treatment objective: maintain intraocular pressure low enough to halt optic nerve destruction.
👁️ Open-Angle Glaucoma
⚡ Angle-Closure Glaucoma
PRIMARY OPEN-ANGLE GLAUCOMA
ANGLE-CLOSURE GLAUCOMA
Most Common Form
Acute Risk
The drainage angle remains physically open, but the trabecular meshwork gradually loses efficiency.
The iris physically blocks the drainage angle, causing sudden, dangerous IOP spikes.
IOP rises slowly, painlessly, and without symptoms.
Acute attacks: intense eye pain, blurred vision, halos, headache, nausea.
Up to 40% of optic nerve may be damaged before patient notices vision loss.
A medical emergency requiring immediate care.
Requires lifelong management.
Laser peripheral iridotomy can prevent attacks in at-risk patients.
◆ STANDARD OF CARE
Established Glaucoma Treatments
Treatment follows a clear escalating hierarchy — from medications to laser to surgery — with most patients requiring lifelong management.
Because glaucoma causes no pain and steals vision gradually, consistent adherence to therapy is the single most important factor in preserving sight.
Step 1 | Prescription Eye Drops — First-Line Therapy
The cornerstone of glaucoma management.
Each drug class works differently: prostaglandin analogs increase uveoscleral outflow; beta-blockers reduce aqueous humor production; carbonic anhydrase inhibitors decrease fluid secretion; alpha-2 agonists reduce production and increase drainage.
Drops are instilled once or twice daily — and adherence is non-negotiable.
Gaps in treatment, even brief ones during fasting, create windows of uncontrolled pressure that cause silent, permanent damage.
Prostaglandin Analogs — increase uveoscleral outflow (e.g., latanoprost, bimatoprost)
Beta-Blockers — reduce aqueous humor production (e.g., timolol)
Carbonic Anhydrase Inhibitors (topical) — decrease fluid secretion (e.g., dorzolamide, brinzolamide)
Alpha-2 Agonists — reduce production and increase drainage (e.g., brimonidine)
Step 2 | Laser Therapy — Targeted Pressure Reduction
Selective laser trabeculoplasty (SLT) stimulates trabecular meshwork drainage in open-angle glaucoma and is increasingly used as primary therapy.
Laser peripheral iridotomy bypasses the blocked drainage angle in angle-closure disease.
Both are outpatient procedures with rapid recovery and favorable safety profiles.
Step 3 | Surgery — When Medical Therapy Falls Short
Trabeculectomy (filtering surgery) and minimally invasive glaucoma surgery (MIGS) are reserved for cases where IOP remains uncontrolled despite maximal medical and laser therapy.
MIGS procedures — including trabecular bypasses, suprachoroidal stents, and micro-shunts — carry substantially lower risk profiles than traditional surgery with faster recovery times.
◆ CLINICAL RESEARCH
How Fasting Really Affects Intraocular Pressure
The research picture on fasting and IOP is more complex — and clinically more interesting — than a simple 'fasting lowers eye pressure' summary. Studies conducted during Ramadan reveal a dynamic, sometimes contradictory pattern that depends critically on the time of day.
📊 Key Clinical Findings
Studies tracking IOP across four weeks of Ramadan fasting in glaucoma patients and healthy controls found:
→ ↓ Overall gradual IOP decrease during fasting period
→ ↑ 4PM — Elevated afternoon IOP in glaucoma patients, higher than post-Ramadan readings
→ ↓ Diurnal — Reduced daily IOP variation in glaucoma patients during fasting
→ +1 week — IOP returns to pre-fasting baseline within one week of resuming normal eating
→ ↑ AM — Heavy water loading at Suhoor can cause transient morning IOP spike
⏰ The Afternoon IOP Problem — Clinically Important
While overall IOP tends to decrease during Ramadan fasting, one study found glaucoma patients had higher IOP readings at 4 PM compared to post-Ramadan measurements, and a reduced diurnal IOP decline throughout the day.
IOP fluctuation — not just average pressure — is a recognized risk factor for glaucoma progression.
A single morning reading does not capture this afternoon elevation.
💧 The Rehydration IOP Spike — A Clinically Overlooked Risk
Rapidly consuming a large volume of water after sunset (Iftar) can cause a transient but significant IOP spike — particularly dangerous for patients with advanced optic nerve damage.
The sudden osmotic load dilutes plasma, transiently reversing the osmolality gradient that was suppressing aqueous humor production.
Key guidance:
→ Pace your fluid intake — sip water steadily over the evening, not all at once
→ Avoid the common Iftar pattern of rapidly consuming cold water, juices, and soups in quick succession
→ Patients with advanced glaucoma or target pressures of 10–12 mmHg should be especially mindful
→ Starting with a moderate amount of water and a few dates at Iftar is consistent with Sunnah practice and sound ophthalmological guidance
Why Does Fasting Alter IOP?
Multiple physiological mechanisms are at work simultaneously — explaining the mixed and time-dependent results in studies:
Plasma Osmolality: Reduced water intake increases plasma osmolality, drawing fluid out of the eye and reducing aqueous humor volume — the primary driver of IOP reduction during fasting
Prostaglandin Fluctuations: Dehydration and dietary changes alter prostaglandin levels, influencing aqueous humor production rates and drainage — contributing to IOP variability
Hormonal Shifts: Fasting alters cortisol, melatonin, and epinephrine rhythms, all of which modulate ocular blood flow and IOP throughout the day
Corneal Biomechanics: Dehydration can alter corneal hydration and fibril spacing, affecting tonometry accuracy — some apparent IOP
changes may reflect measurement artifact
Suhoor Water Loading: Heavy fluid intake at the predawn meal can transiently increase IOP in the morning hours
⚠️ Dehydration Is Not a Treatment Strategy
⚠ The IOP-lowering effect of dehydration is entirely transient — it reverses within days. It provides zero lasting therapeutic benefit.
⚠ Reduced blood pressure from dehydration can lower optic nerve perfusion pressure — a known independent risk factor for progression, particularly in Normal Tension Glaucoma.
⚠ Nocturnal hypotension combined with fasting-related volume depletion may reduce optic nerve blood supply during sleep — the period of greatest vulnerability.
⚠ Prostaglandin fluctuations during fasting contribute to IOP variability throughout the day, not just a simple reduction.
◆ BIOLOGICAL PATHWAYS
Fasting's Potential Protective Mechanisms
Beyond acute IOP changes, intermittent fasting activates systemic biological pathways relevant to glaucoma's neurodegenerative dimension — mechanisms that operate completely independently of eye pressure.
🧠 Neuroprotection of Retinal Ganglion Cells
Glaucoma involves the progressive death of retinal ganglion cells (RGCs) and degeneration of their axons in the optic nerve — a neurodegenerative process similar to Alzheimer's and Parkinson's disease.
Fasting may protect these cells through:
Elevated BDNF (brain-derived neurotrophic factor), supporting neuronal survival and axonal maintenance
Reduced oxidative stress — a key driver of RGC apoptosis and progressive nerve fiber layer thinning
Enhanced mitochondrial biogenesis and function in neural tissue, counteracting energy deficits in the glaucomatous optic nerve
Stimulation of autophagy — the cellular clearance process that removes damaged proteins linked to neurodegeneration
🔥 Anti-Inflammatory Effects in the Retina
Neuroinflammation contributes to optic nerve injury in glaucoma independently of IOP. Animal studies have directly measured fasting's impact on retinal inflammation:
Fasting (3x per week protocol) significantly downregulated TNFa and IL-1b in both retinal tissue and serum in autoimmune glaucoma mouse models
RGCs were measurably protected from damage in fasted animals vs. controls
Systemic reduction in CRP and IL-6 supports healthy microcirculation to the optic nerve head
Attenuated microglial activation in the retina reduces immune-mediated damage to RGCs
🩸 Metabolic Health & IOP Regulation
Metabolic syndrome and chronic hyperinsulinemia are associated with elevated IOP.
High insulin levels may impair trabecular meshwork function and increase aqueous production.
Fasting's metabolic benefits include:
Improved insulin sensitivity — reducing hyperinsulinemia associated with higher IOP
Lower fasting glucose and HbA1c, reducing glycation damage to trabecular meshwork cells
Metformin (a caloric restriction mimetic) has shown association with reduced open-angle glaucoma risk in retrospective studies of diabetic patients
Better blood pressure control supports stable optic nerve perfusion pressure
◆ HIGH-RISK PATIENT GROUPS
Special Cases: Oral Medications & Normal Tension Glaucoma
Two clinical scenarios require particular attention during any fasting period — and both are frequently underemphasized in general glaucoma-and-fasting guidance.
💊 Acetazolamide (Diamox): The Oral Medication Problem
While topical eye drops are confirmed fast-safe, a significant subset of glaucoma patients are prescribed oral acetazolamide (Diamox) tablets.
This is an entirely different clinical situation:
IT BREAKS THE FAST.
As an oral medication, acetazolamide unambiguously invalidates fasting under all major scholarly rulings.
IT IS DANGEROUS TO TAKE WHILE FASTING.
→ Acetazolamide is a diuretic — it actively drives fluid and electrolyte loss through the kidneys
→ Taking it while unable to drink creates compounded dangerous dehydration: drug accelerates fluid loss that cannot be replaced until Iftar
→ Risk of severe electrolyte imbalances (low potassium and bicarbonate), metabolic acidosis, and kidney stress
→ Significant blood pressure drops can compromise optic nerve perfusion
→ Clinical guidance: Patients on oral acetazolamide almost universally qualify for the medical (darurat) exemption from fasting.
Discuss switching to topical carbonic anhydrase inhibitor drops with your ophthalmologist.
🫀 Normal Tension Glaucoma (NTG): When Blood Flow Matters More Than Eye Pressure
In NTG, the primary driver of nerve damage is impaired vascular supply to the optic nerve head — not elevated pressure.
This makes NTG patients a distinctly higher-risk group during fasting, and for reasons quite different from pressure-driven glaucoma.
→ Fasting-related drops in systemic blood pressure — particularly during sleep — can reduce optic nerve perfusion pressure to levels that accelerate NTG damage
→ Many NTG patients already experience problematic nocturnal BP dips. Dehydration and reduced caloric intake can worsen this, extending overnight windows of reduced optic nerve blood flow
→ NTG patients on systemic antihypertensives face compounded risk: drug effect plus fasting-related hypotension can produce excessively low nocturnal readings
→ For NTG patients, the IOP changes from fasting are less clinically relevant than the hemodynamic changes
→ Recommendation: Discuss fasting explicitly with your ophthalmologist.
Ask whether 24-hour ambulatory blood pressure monitoring (ABPM) is appropriate before Ramadan
◆ RESEARCH REVIEW
Human Data vs. Animal Models: An Honest Assessment
It is essential to distinguish what has been shown in animal experiments versus established in human populations.
Both matter — but they answer different questions.
👤 Human Studies
🐭 Animal Models
HUMAN STUDIES
ANIMAL MODELS
Large NHANES analysis (7,081 participants): habitual breakfast skipping does not reduce diagnosed glaucoma risk in older adults
Intermittent fasting (3x/week) significantly protected RGCs in autoimmune glaucoma mouse models
Glaucoma risk most strongly predicted by age and racial identity (Black, Hispanic/Latino populations), not dietary timing
Pro-inflammatory cytokines TNFa and IL-1b were directly downregulated in retinal tissue and serum
IOP reductions during Ramadan are real but transient — reverting within one week of normal eating
Dietary restriction consistently showed neuroprotective effects on the optic nerve
Some studies show higher afternoon IOP in glaucoma patients during fasting — mixed results overall
Anti-inflammatory mechanisms are well-characterized in experimental models
No long-term human trial demonstrates fasting prevents glaucoma onset or slows progression
Promising mechanistic data — human clinical translation not yet established
The honest scientific position: fasting holds real mechanistic promise as an adjunct — but does not substitute for pressure-lowering therapy, and current human evidence does not support it as a standalone glaucoma prevention strategy.
◆ SPECIAL CLINICAL FOCUS
Ramadan Fasting: Medications, Faith & Eye Safety
For millions of Muslim patients with glaucoma worldwide, Ramadan creates a recurring and preventable clinical crisis: patients stopping their eye drops out of fear that the medication invalidates the fast.
Research identifies this behavioral risk — not any physiological effect of fasting — as the primary safety concern in this population.
The 'Taste' Problem & Why It Matters
Eye drops drain through the nasolacrimal duct and can be tasted at the back of the throat. Many patients interpret this as evidence that something has entered their stomach — and stop their treatment entirely.
The International Glaucoma Association warns: stopping drops, even briefly, can cause permanent, irreversible vision loss — because by the time patients notice damage, 40% of their sight may already be gone.
Islamic Rulings on Eye Drops
Multiple major Islamic scholarly bodies have confirmed that topical eye drops do not invalidate the fast:
Egyptian Dar al-Ifta — one of the oldest and most respected Islamic legal bodies — confirms drops are permissible
Muslim Council of Britain — has explicitly addressed this in glaucoma patient guidance with the International Glaucoma Association
British Islamic Medical Association (BIMA) — has published clinical and religious guidance confirming topical drops are fast-safe
Mufti Wilayah Persekutuan (Malaysia) — has issued rulings permitting eye drops and providing exemption guidance for oral medications
Punctal Occlusion — The Practical Solution
Applying gentle finger pressure to the inner corner of the eye (tear duct) for 1–2 minutes after instilling drops blocks nasolacrimal drainage.
This eliminates the throat taste, removes religious concern, and improves drug bioavailability — making it best practice for ALL glaucoma patients, not just those fasting.
Suhoor & Iftar Scheduling
For patients who remain doubtful, drops can typically be rescheduled to align with predawn (Suhoor) and sunset (Iftar) — outside fasting hours — under ophthalmologist supervision.
Long-acting formulations may offer additional flexibility.
Medical Exemption (Darurat)
If fasting poses a direct threat to organ function — for example, where oral medications (acetazolamide) require continuous hydration to prevent kidney damage — Islamic law permits and in some rulings mandates breaking the fast.
Patients with chronic unrecoverable conditions may pay fidyah (feeding the poor) instead of making up missed days.
"Islam advocates that people take care of their bodies... stopping drops even for a short period of time can cause permanent loss of vision."
— International Glaucoma Association / Muslim Council of Britain
◆ FOR PATIENTS & CLINICIANS
Clinical Protocol: Fasting Safely with Glaucoma
Whether fasting for religious observance or metabolic health, glaucoma patients need a clear, individually tailored plan.
The following recommendations synthesize clinical study findings and published guidelines:
Area
Recommendation & Clinical Rationale
Eye Drops
Never stop or reduce prescribed eye drops during fasting. Eye drops do not break the fast.
Use punctal occlusion (pressure on tear duct for 1–2 min) to eliminate nasolacrimal drainage and the associated throat taste.
Hydration
Consume 8–10 cups of water between Iftar and Suhoor — but sip gradually.
Rapid rehydration at Iftar can cause a transient IOP spike. Adequate, paced hydration maintains optic nerve perfusion pressure and stabilizes systemic blood pressure overnight.
Medication Timing
Reschedule drops to Suhoor and Iftar if possible, under physician supervision.
Note: oral acetazolamide (Diamox) breaks the fast and is dangerous during fasting — discuss switching to topical CAI drops or medical exemption.
Diet During Non-Fasting Hours
Prioritize water-rich fruits and vegetables.
Avoid diuretics (coffee, tea, excess salt) that accelerate fluid loss and worsen IOP variability and nocturnal blood pressure instability.
IOP Monitoring
Increase monitoring frequency during fasting — especially for unstable or advanced disease.
A normal morning reading does not guarantee stability throughout the day: the afternoon IOP elevation pattern requires time-of-day-specific monitoring.
Advanced Glaucoma
Patients with target pressure of 10–12 mmHg have minimal buffer for fluctuations.
Fasting-related IOP spikes (including Iftar rehydration spikes) may be especially significant.
Lower threshold for seeking review.
Blood Pressure / NTG
Monitor blood pressure, particularly nocturnal readings, if taking antihypertensives alongside glaucoma drops. NTG patients: nocturnal hypotension is a primary risk factor — consider ABPM monitoring before and during Ramadan.
Planned Procedures
If you have a scheduled laser treatment (SLT, iridotomy) or surgical procedure during a fasting month, inform your care team in advance.
Perioperative hydration and medication timing may need adjustment.
Red Flag Symptoms
Break the fast immediately and seek urgent review for: sudden vision changes, severe eye pain, persistent headache, halos around lights with nausea (acute angle-closure), or persistent dizziness.
Fasting Duration
For elective intermittent fasting (non-religious), a 12–16 hour eating window is a reasonable starting point. Extended fasts carry greater hemodynamic risk and should only be undertaken with ophthalmologist input.
Do This. Not That.
✓ DO
✗ DON'T
Continue eye drops exactly as prescribed
Stop or skip medications to 'preserve' the fast
Discuss fasting plans with your ophthalmologist beforehand
Drink a large volume of water all at once when breaking the fast
Use punctal occlusion technique after every drop
Assume all fasting protocols are safe for your specific case
Pace fluid intake gradually after Iftar — sip steadily, don't gulp
Apply drops carelessly — nasolacrimal drainage increases systemic absorption
Stay well hydrated across the full non-fasting window
Ignore new or worsening eye symptoms
Seek religious guidance — scholarly consensus permits eye drops
Feel pressured to fast if medically inadvisable
Monitor IOP at multiple times of day, not just morning
Treat a normal morning IOP as proof of stability all day
Tell your surgical team if you have a procedure during a fasting month
Use dehydration as a deliberate IOP-lowering strategy
Report new symptoms promptly
Take oral acetazolamide without discussing religious exemption with your doctor and scholar
◆ THE BOTTOM LINE
Glaucoma & Fasting: What the Expert Evidence Says
Fasting with glaucoma is possible for most patients — but it demands careful pre-planning, uninterrupted medication, and an awareness of nuances that generic guidance misses.
The central message remains medication compliance: eye drops are permitted by all major Islamic scholarly authorities, and stopping them risks silent, permanent vision loss.
The expert clinical picture adds important layers: the rehydration IOP spike risk at Iftar, the unique vascular hazard for Normal Tension Glaucoma patients, the serious dehydration danger for those on oral acetazolamide, the importance of pacing fluids rather than gulping, and the need to inform surgical teams about fasting schedules.
Fasting's potential neuroprotective and anti-inflammatory benefits are biologically real — but remain experimentally promising rather than clinically proven in humans.
Area
Recommendation & Clinical Rationale
Core Treatment (Non-Negotiable)
Daily prescription eye drops always | Laser therapy when indicated | Surgery if uncontrolled | Regular IOP monitoring | Optic nerve imaging (OCT / Visual Fields)
Key Fasting Risks
Medication non-compliance (#1 risk) | Rapid rehydration IOP spike at Iftar | Acetazolamide + dehydration danger | NTG: nocturnal BP dips | Afternoon IOP elevation pattern
Safety Protocol
Never stop drops — they are permitted | Punctal occlusion every time | Sip water steadily — don't gulp at Iftar | Monitor afternoon IOP, not just AM | NTG patients: track nocturnal blood pressure
Medical Disclaimer
This document is for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment.
Glaucoma is a serious, progressive condition requiring individualized clinical management.
Always consult your ophthalmologist before making any changes to your treatment plan or lifestyle, including fasting.
For religious guidance on fasting with medical conditions, consult a qualified Islamic scholar alongside your physician.
Therapeutic Fasting Approach for Eye Conditions by Dr. Hassan Al-Warraqi
This document outlines a structured approach to therapeutic fasting, proposed as a supportive metabolic strategy for eye conditions, aiming to complement standard ophthalmic care.
This approach is primarily discussed in the context of chronic systemic or inflammatory conditions and may be considered for patients with certain eye diseases under strict medical supervision.
1. Fasting Pattern
The proposed fasting regimen typically follows one of two distinct schedules, designed to stimulate metabolic switching, enhance insulin sensitivity, and alleviate inflammatory signaling:
Option A: Intermittent Therapeutic Fasting
Frequency: Fasting is undertaken for 3-4 days per week.
Distribution: Non-consecutive days are generally preferred to allow for periods of normal food intake.
Eating Days: Regular food intake is maintained on non-fasting days.
Option B: Daily Intermittent Fasting
Frequency: Fasting is observed every day within a strictly defined time window.
Duration: This option involves extended fasting hours, similar to practices during Ramadan or through time-restricted feeding protocols.
2. Continuation of Medications
A fundamental principle of this therapeutic approach is the uninterrupted continuation of all prescribed medications.
For eye patients, this includes, but is not limited to:
Intraocular pressure-lowering eye drops.
Anti-inflammatory medications.
Antibiotics, when clinically necessary.
Systemic medications prescribed by other physicians.
It is critically important not to discontinue treatment regimens, especially in conditions like glaucoma where consistent pressure control is vital for preserving vision.
3. Timing of Surgery or Procedures
For patients undergoing eye procedures, adjustments to the fasting regimen are essential:
Pause Before Procedure: Fasting may be temporarily suspended during the period immediately preceding the procedure.
Types of Procedures: This includes procedures such as laser therapy, intravitreal injections, and various types of eye surgery.
Resuming Fasting: The fasting regimen is typically resumed after a recovery period of approximately two days post-procedure.
This period is crucial for ensuring stable hydration, facilitating wound healing, and maintaining adherence to medication schedules.
4. Potential Physiological Rationale
Proponents of therapeutic fasting suggest several potential physiological mechanisms that might contribute to its supportive role in eye health:
Reduction of Systemic Inflammation: Fasting can lead to a decrease in systemic inflammatory markers.
Improved Metabolic Regulation: It can enhance metabolic processes, including glucose and lipid metabolism.
Enhancement of Cellular Repair Pathways: Fasting is known to activate autophagy, a vital cellular process for removing damaged cells and promoting cellular renewal.
Better Vascular Function: Improvements in vascular health can indirectly benefit eye tissues, especially in diseases with a vascular component.
These effects are hypothesized to indirectly influence eye health, particularly in conditions linked to systemic vascular or metabolic dysfunction.
5. Application in Ophthalmology Contexts
This approach has been discussed in the context of various eye diseases, including:
Glaucoma management support.
Retinal vascular conditions.
Inflammatory eye diseases.
Metabolism-related eye disorders.
However, the application of fasting must always be highly individualized, especially for patients with:
Unstable glaucoma.
Recent eye surgery.
Severe systemic disease.
High risk of dehydration.
6. Clinical Caution
It is essential to emphasize that therapeutic fasting is not a substitute for evidence-based ophthalmic care.
It should only be considered as a complementary lifestyle intervention and must always be undertaken under the guidance and direct supervision of a qualified medical professional.
Regular monitoring of key ophthalmic parameters remains essential, including:
Intraocular pressure (IOP).
Visual fields.
Optic nerve status.
This vigilant monitoring ensures the patient's eye health is maintained and any potential adverse effects of fasting are promptly identified and managed.
Glaucoma and Fasting: Frequently Asked Questions (FAQs)
1. Does using eye drops break my fast?
Generally, no.
Eye drops are considered permissible by most religious and medical authorities because they are applied topically and do not involve consuming a substance through the digestive tract.
2. I can taste the drops sometimes. Does that break the fast?
If you taste the drops, it can feel like you have consumed something. To prevent this, use a technique called punctal occlusion.
After putting a drop in your eye, gently press on the inner corner of your eye (near your nose) for one to two minutes.
This blocks the tear duct, stopping the medication from draining into your throat and keeping it in your eye longer.
3. Can I just change when I take my eye drops?
You should never change your medication schedule on your own.
However, you can work with your doctor to adjust the timing.
The goal is to align your doses with your pre-dawn (Suhoor) and post-dusk (Iftar) meals.
Your ophthalmologist can advise if this schedule will maintain stable pressure control for your specific condition.
4. Is it safe to fast if I have diabetes and glaucoma?
It requires extra caution, especially if you are taking beta-blocker eye drops (like timolol).
These drops can mask the typical warning signs of low blood sugar (hypoglycemia), such as a rapid heartbeat.
If you have diabetes, you must consult both your ophthalmologist and primary care doctor before fasting.
5. I heard fasting lowers eye pressure. Can I stop my medication while fasting?
Absolutely not. While research shows fasting can lower intraocular pressure (IOP), it does not replace the need for prescribed medication.
The effect of your eye drops is stronger and more consistent.
Stopping your drops can lead to dangerous pressure spikes and permanent vision loss.
Think of fasting as a potential additional benefit, not a substitute for treatment.
6. What should I do if I miss my pre-dawn dose?
If you forget to take your drops at Suhoor, do not take them during the day.
Wait until your evening meal (Iftar) to take your scheduled dose.
Do not double your dose to make up for the missed one. Simply resume your normal schedule at the next permitted time.
7. What specific symptoms should make me break my fast?
You should break your fast and seek immediate medical attention if you experience:
Severe eye pain.
A sudden and significant decrease in vision.
Nausea or vomiting accompanied by eye pain.
Any symptoms of a very low blood sugar reaction (if diabetic), like severe sweating, confusion, or dizziness.
8. I have Normal Tension Glaucoma.
Is there anything special I should know?
Yes.
In Normal Tension Glaucoma, eye pressure is often not elevated, but blood flow to the optic nerve may be a factor.
Fasting can affect your blood pressure.
Your doctor might recommend monitoring your blood pressure at home during the fast to ensure it is not dropping too low, which could potentially impact optic nerve health.
===================================================================================================================================================================================================
👁️🌙 Eye Health, Glaucoma & Fasting Protocols · A Scientific Overview
https://www.h-k-e-m.com/-eye-health-glaucoma-and-fasting-protocols-a-scientific-overview
glaucoma and fasting, intraocular pressure during fasting, eye health Ramadan, fasting and optic nerve, dehydration and eye pressure, intermittent fasting eye health, glaucoma management guidelines, ophthalmology fasting protocol, neuroprotection and fasting, clinical guidance glaucoma
Glaucoma involves degeneration of retinal ganglion cells and optic nerve fibers. Elevated IOP remains the primary modifiable risk factor, yet many patients continue to progress despite normal pressure levels, highlighting vascular and metabolic influences.
Fasting represents a promising adjunct strategy targeting metabolic and neurodegenerative pathways implicated in glaucoma. While not a cure, it may enhance systemic and ocular resilience when integrated safely with evidence-based medical care.
===================================================================================================================================================================================================
===================================================================================================================================================================================================


Get in touch
Address
Cairo Al Rehab
Contacts
+20 109 405 2056
hassanalwarraqi@h-k-e-m.com