
Health is a crown on the heads of the healthy that only the sick can see.


⚖️Weight Loss Drugs Tirzepatide, Semaglutide & Fasting🌙
Compare tirzepatide, semaglutide, and intermittent fasting for weight loss — clinical data, safety risks, discontinuation rates, and when to combine drug therapy with fasting.
FASTINGWEIGHT LOSS DRUGS
Dr Hassan Al Wwarraqi
7/15/202612 min read
⚖️Weight Loss Drugs Tirzepatide, Semaglutide & Fasting🌙
Compare tirzepatide, semaglutide, and intermittent fasting for weight loss — clinical data, safety risks, discontinuation rates, and when to combine drug therapy with fasting.
tirzepatide vs semaglutide
intermittent fasting vs calorie restriction, GLP-1 weight loss drugs, modified alternate-day fasting, weight loss medication side effects
Tirzepatide vs Semaglutide and Fasting: Weight Loss Options in 2026
As global obesity rates climb, two very different strategies have taken center stage in weight management: GLP-1 receptor agonist medications like tirzepatide and semaglutide, and structured fasting protocols such as intermittent fasting (IF).
guide breaks down what the current clinical evidence shows about each approach, their risks, and how they can work together.
How Tirzepatide Compares to Semaglutide
A large propensity-matched cohort study of more than 18,000 patients tracked outcomes over a 12-month treatment period and found a clear, widening advantage for tirzepatide at every weight-loss milestone measured.
Weight Loss Thresholds
5% weight loss: 81.8% of tirzepatide patients achieved this versus 66.5% of semaglutide patients (hazard ratio 1.76)
10% weight loss: 62.1% versus 37.1% (hazard ratio 2.54)
15% weight loss: 42.3% versus 18.1% (hazard ratio 3.24)
The Gap Widens Over Time
The absolute difference in weight reduction grows the longer patients stay on treatment:
At 3 months: an additional 2.4% weight loss with tirzepatide
At 6 months: the gap widens to 4.3%
At 12 months: tirzepatide shows a 6.9% greater absolute reduction in body weight
Notably, weight loss outcomes tend to be more pronounced in patients without Type 2 Diabetes, regardless of which medication is used — a difference attributed to underlying metabolic factors still under investigation.
Intermittent Fasting vs Continuous Calorie Restriction
A systematic review and meta-analysis of randomized controlled trials compared intermittent fasting (IF) to continuous calorie restriction (CCR) in overweight and obese adults.
Body weight: IF produced significantly greater weight loss than CCR (SMD −0.21, p = 0.028).
BMI: No significant difference emerged between the two approaches (SMD 0.02, p = 0.848) — meaning fasting reduces overall weight more, but BMI improvements track similarly either way.
Metabolic markers: Both approaches produced comparable improvements in total cholesterol, triglycerides, and waist circumference.
Not All Fasting Protocols Are Equal
Modified Alternate-Day Fasting (ADF): Involves roughly 75% energy restriction on fasting days. This protocol showed a significant advantage over CCR in both weight and BMI reduction, making it the standout regimen in the review.
Standard intermittent fasting (2 days/week): Showed no significant advantage over CCR in some studies, underscoring that fasting intensity and frequency matter as much as the fasting concept itself.
Why Fasting Works: The Biological Mechanisms
Intermittent fasting appears to work by inhibiting anabolic processes and improving mitochondrial energy metabolism, with several specific pathways involved:
Glucose regulation: IF enhances glucose uptake in peripheral tissues while suppressing gluconeogenesis, favoring fat oxidation.
Adipose tissue browning: Certain fasting patterns (one fasting day followed by two feeding days) promote conversion of energy-storing white fat into metabolically active brown fat.
Muscle preservation: Some evidence suggests IF may better preserve lean body mass compared to standard calorie-restricted diets.
Who Should Avoid Aggressive Fasting
For adults over 60, continuous calorie restriction is generally considered safer than aggressive fasting protocols, since older adults often have reduced metabolic capacity and lower tolerance for extended hunger. Extreme intermittent restriction may pose unnecessary physiological stress in this group.
Common Side Effects
Muscle pain, sleep disturbances, headaches, and intense hunger are the most frequently reported symptoms, typically appearing in the first few days of a fasting protocol and stabilizing as the body adapts.
what drugs can help lose weight
FDA-approved weight-loss drugs fall into two main categories: highly effective GLP-1 and GIP receptor agonists (like semaglutide and tirzepatide) and older oral stimulants .
To be prescribed these medications, you typically need a Body Mass Index (BMI) over 30, or a BMI over 27 with a weight-related health condition.
GLP-1 & Dual Agonists These medications mimic gut hormones to slow digestion, reduce appetite, and silence food cravings.
Semaglutide (Wegovy): A weekly injection (or daily oral pill) proven to cause significant weight loss and lower the risk of cardiovascular events.
Safety Considerations for GLP-1 Medications
GLP-1 receptor agonists — including semaglutide, tirzepatide, liraglutide, and dulaglutide — share a similar adverse-event profile.
Most common: Nausea, vomiting, diarrhea, and constipation, which are often dose-dependent and improve over time.
Serious risks requiring monitoring:
Pancreatitis — rare, occurring in an estimated 0.3–0.5% of trial participants
Gallbladder disease, including gallstones and cholecystitis, potentially worsened by rapid weight loss
Thyroid risk — a boxed warning exists based on animal studies; these drugs are contraindicated in patients with a personal or family history of medullary thyroid carcinoma or MEN2
Kidney function — acute kidney injury is a possibility, so eGFR testing is recommended before starting treatment
The Discontinuation Problem
One of the biggest challenges facing GLP-1 therapy is treatment persistence.
Within the study follow-up period, 55.9% of tirzepatide patients and 52.5% of semaglutide patients discontinued therapy — meaning roughly half of all patients are off medication within a year.
how much overweight to get ozempic
To qualify for Ozempic or similar weight-loss medications like Wegovy, you generally need a Body Mass Index (BMI) of 30 or higher (obese), or a BMI of 27 or higher combined with at least one weight-related condition such as type 2 diabetes, high blood pressure, or sleep apnea.
Ozempic is technically FDA-approved for managing type 2 diabetes, but doctors often prescribe it off-label for weight management based on these BMI thresholds.
Wegovy, which contains the same active ingredient (semaglutide) but is formulated specifically for weight loss, uses these exact BMI guidelines.
Why Patients Stop
High out-of-pocket costs
Persistent gastrointestinal side effects
Drug supply shortages
Perceived lack of benefit
The complexity of injection-based dosing and titration
What Happens After Stopping
Abrupt discontinuation is frequently followed by rapid weight regain (often exceeding pre-treatment baseline within months), glycemic relapse in diabetic patients, and metabolic rebound affecting insulin sensitivity and lipid profiles.
Medical supervision for tapering — or transitioning to an alternative strategy — is strongly recommended.
Fasting as an Alternative or Bridge Strategy
Given how many patients discontinue GLP-1 therapy, structured fasting protocols — particularly modified ADF — offer a viable primary or adjunctive option for patients who can't access, afford, or tolerate medication.
Fasting may also help maintain weight loss and blunt the rebound effect for patients transitioning off drug therapy.
Combining Medication and Fasting
For some patients, pairing a GLP-1 medication with intermittent fasting may offer synergistic benefits: the appetite suppression from the drug can make fasting windows easier to tolerate, while fasting-induced metabolic adaptations may enhance the medication's insulin-sensitizing and fat-oxidizing effects.
This combination requires close medical supervision to avoid excessive caloric restriction, muscle loss, or nutrient deficiencies.
weight loss drugs for men
can anyone take ozempic to lose weight
Not everyone can—or should—take Ozempic .
While weight loss is a common side effect, Ozempic is FDA-approved specifically for managing type 2 diabetes and reducing cardiovascular risks, not for weight loss.
Physicians may prescribe it "off-label" for weight management.
According to clinical consensus and medical guidelines, you typically qualify if you have: A Body Mass Index (BMI) of 30 or higher (obesity).
A BMI of 27 or higher with weight-related health conditions (like high blood pressure or high cholesterol).
A healthcare provider must evaluate your complete medical history
Choosing the Right Path
Consider medication if you:
Have severe obesity requiring rapid, clinically meaningful weight loss
Have Type 2 Diabetes needing concurrent glycemic control
Have not responded to dietary interventions alone
Have obesity-related comorbidities where drug-induced weight loss reduces cardiovascular risk
Consider fasting if you:
Have contraindications to GLP-1 therapy (thyroid history, pancreatitis, severe GI disease)
Want a cost-effective, non-pharmacological approach
Are concerned about long-term drug dependency or discontinuation rebound
Are over 60 and may do better with moderate, sustained calorie restriction than aggressive fasting or medication
The Bottom Line
Both GLP-1 receptor agonists and structured fasting protocols represent legitimate, evidence-based paths to meaningful weight loss — but neither is a one-size-fits-all solution.
Successful outcomes depend on proper pre-treatment screening, active management of side effects, realistic expectations, and a clear plan for long-term maintenance, whichever path — or combination — a patient and their physician choose.
Frequently Asked Questions: Tirzepatide vs Semaglutide and Fasting for Weight Loss FAQs About Weight Loss Medications
What is the difference between tirzepatide and semaglutide?
Tirzepatide and semaglutide are both weight loss medications, but they differ in mechanism of action and effectiveness.
Tirzepatide is a dual GLP-1/GIP agonist, meaning it targets two hormonal receptors instead of one. Semaglutide is a GLP-1 receptor agonist only. In large-scale clinical studies, tirzepatide demonstrated significantly superior weight loss outcomes:
5% weight loss: 81.8% with tirzepatide vs. 66.5% with semaglutide
10% weight loss: 62.1% with tirzepatide vs. 37.1% with semaglutide
15% weight loss: 42.3% with tirzepatide vs. 18.1% with semaglutide\
Is tirzepatide better than semaglutide for weight loss?
Yes, based on current clinical evidence, tirzepatide outperforms semaglutide across all measured weight loss thresholds.
The gap widens over time, reaching a -6.9% absolute difference in total body weight reduction after 12 months.
However, medication selection should always be individualized and under medical supervision.
What are the most common side effects of GLP-1 medications?
The most frequently reported adverse effects are gastrointestinal symptoms:
Nausea
Vomiting
Diarrhea
Constipation
These symptoms are often dose-dependent and tend to improve over time. Gradual dose titration helps minimize their severity.
Are there serious risks from taking tirzepatide or semaglutide?
Yes, although rare, there are serious risks requiring medical monitoring:
Pancreatitis: A rare (~0.3–0.5% in trials) but serious risk requiring immediate attention.
Gallbladder Disease: Includes gallstone formation and cholecystitis, particularly with rapid weight loss.
Thyroid Risks: Boxed warnings exist due to animal studies.
Contraindicated for individuals with a personal or family history of medullary thyroid carcinoma or MEN2.
Kidney Issues: Potential for acute kidney injury. eGFR testing is recommended before starting treatment.
Why do so many patients stop taking GLP-1 medications?
Studies show that approximately 50% of patients discontinue therapy within one year.
The primary drivers are:
High cost and financial burden
Persistent gastrointestinal side effects
Drug shortages and access difficulties
Perceived lack of expected results
Complexity of injection-based administration
What happens when you stop tirzepatide or semaglutide?
Abrupt discontinuation frequently leads to:
Rapid weight regain: Often exceeding pre-treatment baseline within months
Glycemic relapse: For diabetic patients, blood sugar control deteriorates quickly
Metabolic rebound: Worsening insulin sensitivity and lipid profiles
Medical supervision with a tapering protocol is always recommended.
Can you combine medications with intermittent fasting?
Yes, combining approaches may offer synergistic benefits.
Medications suppress appetite making fasting easier, while fasting enhances metabolic adaptations. However, this requires close medical supervision to avoid:
Excessive caloric restriction
Muscle loss
Nutrient deficiencies
FAQs About Intermittent Fasting
What is intermittent fasting?
Intermittent Fasting (IF) is an eating pattern that cycles between periods of fasting and eating. Unlike diets that specify what to eat, intermittent fasting focuses on when you eat.
Is intermittent fasting better than continuous calorie restriction?
Meta-analysis data shows that intermittent fasting leads to greater weight loss (SMD = -0.21, p = 0.028) compared to continuous calorie restriction.
However, no significant difference was found in BMI reduction.
Both approaches improve cholesterol, triglycerides, and waist circumference comparably.
What is the best intermittent fasting protocol?
Modified Alternate-Day Fasting (ADF) is the most effective protocol.
It involves consuming only 25% of usual calories on fasting days (75% restriction).
This pattern demonstrated significant advantages in both weight loss and BMI reduction over continuous calorie restriction.
How does intermittent fasting work for weight loss?
Intermittent fasting operates through several biological mechanisms:
Glucose Regulation: Enhances sugar uptake in tissues and prevents new glucose formation in the liver
Fat Transformation: Converts white fat (storage) into brown fat (energy-burning)
Muscle Preservation: May be superior at maintaining lean mass while reducing fat mass
Mitochondrial Improvement: Enhances cellular energy metabolism
What are the side effects of intermittent fasting?
Common symptoms, especially in the initial days:
Muscle pain
Sleep disturbances
Headaches
Intense hunger
These effects typically stabilize as the body adapts to the new eating pattern.
Is intermittent fasting safe for everyone?
No. It may be harmful for certain populations:
Adults over 60: Moderate continuous calorie restriction is preferred
Pregnant and breastfeeding women
Diabetic patients (without medical supervision)
Individuals with a history of eating disorders
Can fasting replace weight loss medications?
For patients who cannot afford or tolerate medications, intermittent fasting represents an effective alternative.
Modified ADF delivers statistically significant results.
It can also be used as a supplement or during medication transitions to prevent weight regain.
Comparative FAQs: Medications vs. Fasting
Which is better: medications or intermittent fasting?
There is no one-size-fits-all answer.
The choice depends on individual circumstances:
Choose medications if:
You have severe obesity
You have Type 2 Diabetes
You have failed dietary interventions alone
You have serious obesity-related complications
Choose fasting if:
You seek a non-pharmacological solution
You cannot afford medication costs
You have medical contraindications to drugs
You prefer a natural, long-term approach
Can fasting be used alongside medications?
Yes, the combination may be beneficial. Medications facilitate fasting by suppressing appetite, while fasting amplifies the metabolic benefits of the drugs.
This requires medical supervision to mitigate risks.
Which is more sustainable long-term?
Both face challenges. 50% of medication patients stop within a year due to cost and side effects.
Intermittent fasting requires a lifestyle change that may be difficult initially.
Success depends on commitment and ongoing medical support.
Can you combine intermittent fasting with continuous calorie restriction?
Yes, some patients alternate between approaches.
For example, intermittent fasting on weekdays with moderate restriction on weekends.
Flexibility may improve long-term adherence.
What is your advice for someone starting their weight loss journey?
Consult your doctor first: For screening contraindications and determining the best approach
Start gradually: Whether with medication or fasting, slow escalation reduces side effects
Be realistic: Losing 5-10% of body weight significantly improves health
Plan for maintenance: Consider how you will sustain weight loss before starting
Monitor your health: Regular checks for kidney, pancreatic, and thyroid function
Safety and Monitoring FAQs
What tests are required before starting medication?
eGFR: For kidney function
Pancreatic enzymes: For pancreatic health
Thyroid history: Comprehensive screening
Complete blood count: For cholesterol and blood sugar
Psychological assessment: To rule out eating disorders
How often should I follow up with my doctor?
First month: Every two weeks for monitoring and adjustment
Months 2-3: Monthly visits
After 6 months: Every 3 months
Annually: Comprehensive examinations
What are the warning signs requiring immediate discontinuation?
Severe abdominal pain (possible pancreatitis)
Yellowing of skin or eyes
Difficulty breathing
Swelling of face or throat
Sudden vision changes
Can I exercise while on medication or fasting?
Yes, exercise is recommended with both approaches.
With medications, start gradually to avoid exhaustion.
With fasting, you may need to adjust workout timing to prevent dizziness.
Cost and Access FAQs
How much do tirzepatide and semaglutide cost?
Costs vary by country and insurance, but are generally very high (hundreds to thousands of dollars monthly).
This financial burden is the leading cause of treatment discontinuation.
Does insurance cover these medications?
Coverage is inconsistent.
Some insurance plans cover them for severe obesity or diabetes, but often require:
High BMI (≥30 or ≥27 with complications)
Documentation of previous diet failures
Ongoing medical supervision
Is intermittent fasting free?
Yes, intermittent fasting requires no monetary cost. However, it does require:
Education and guidance (may be paid)
Meal planning
Psychological and social support
Conclusion
Whether you choose tirzepatide, semaglutide, intermittent fasting, or a combination approach, the keys to success are:
Continuous medical supervision
Realistic expectations
Long-term commitment
A clear maintenance plan
Weight loss is not a race, but a journey requiring patience and ongoing adaptation.
==============================================================================================================================================
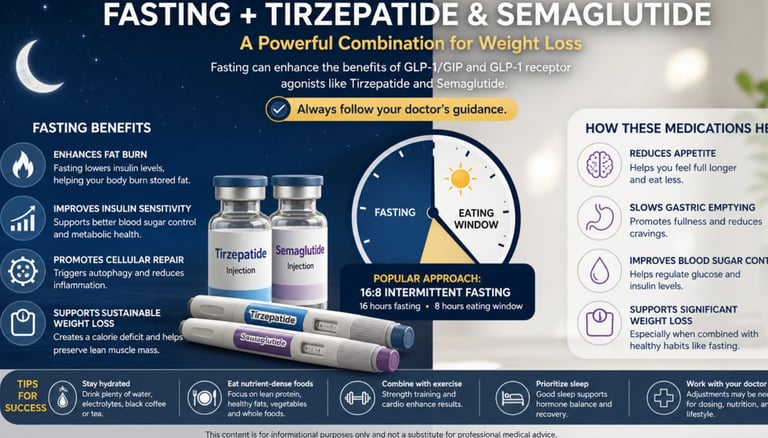
💉⚖️ Tirzepatide vs. Semaglutide for Weight Loss: Which Works Better with Fasting? 🌙
Both tirzepatide and semaglutide are among the most effective medications currently available for treating obesity. They reduce appetite, slow stomach emptying, and improve blood sugar control, making it easier for many people to lose weight.
🏆 Tirzepatide generally produces greater weight loss than semaglutide because it activates both the GIP and GLP-1 receptors, while semaglutide targets only the GLP-1 receptor. In clinical studies, tirzepatide has achieved average weight loss of around 20–22% of body weight, compared with about 15–17% for semaglutide.
🌙 What About Fasting?
Intermittent fasting may complement either medication by:
🔥 Increasing fat burning.
📉 Improving insulin sensitivity.
🍽️ Helping reduce overall calorie intake.
❤️ Supporting better metabolic health.
⚡ Helping some people maintain energy once adapted to fasting.
However, current scientific evidence does not show that fasting dramatically boosts the weight-loss effects of tirzepatide or semaglutide beyond what the medications already achieve. More research is needed.
⚠️ Use Caution
Combining fasting with these medications may increase the risk of:
Dehydration.
Dizziness or lightheadedness.
Low blood sugar, especially if you also take insulin or sulfonylureas.
Nausea, vomiting, constipation, or diarrhea.
Extended fasts should only be undertaken with guidance from a healthcare professional, particularly for people with diabetes or other chronic medical conditions.
✅ Bottom Line
If the goal is maximum weight loss, tirzepatide currently has the strongest evidence for greater effectiveness.
If the goal is long-term success, the most effective strategy combines medication with:
🌙 A sustainable fasting routine (when medically appropriate).
🥗 A nutritious, calorie-appropriate diet.
🏃 Regular physical activity.
😴 Adequate sleep.
🩺 Ongoing medical follow-up.
Neither medication replaces healthy lifestyle habits, and fasting should be individualized based on a person's health status and medical treatment.
====================================================================================================================================================================================
🧃🍭 Hidden Fructose & Fasting: Can Fasting Reverse Its Harmful Effects?
Hidden fructose lurks in many everyday foods—not just sweets. Soft drinks, fruit-flavored beverages, breakfast cereals, energy drinks, flavored yogurts, ketchup, barbecue sauce, packaged snacks, and many ultra-processed foods often contain added fructose or high-fructose corn syrup (HFCS).
Excessive intake has been linked to insulin resistance, non-alcoholic fatty liver disease (NAFLD), obesity, type 2 diabetes, and cardiovascular disease.
🌙 Can Fasting Help?
Growing evidence suggests that intermittent fasting and time-restricted eating may promote metabolic health by:
✅ Improving insulin sensitivity.
✅ Reducing liver fat, particularly when accompanied by weight loss.
✅ Lowering chronic inflammation and oxidative stress.
✅ Enhancing metabolic flexibility (the body's ability to switch between glucose and fat for energy).
✅ Supporting healthy body weight and blood sugar control.
These benefits may help reduce some of the metabolic effects associated with excessive fructose consumption.
⚠️ What the Evidence Says
While fasting shows promise as a metabolic intervention, there is currently no strong scientific evidence that fasting alone can completely reverse the long-term damage caused by excessive fructose intake.
Lasting improvements depend on addressing the underlying dietary pattern.
🥗 A Smarter Strategy
The best results come from combining fasting—when appropriate—with other healthy habits:
Choose whole fruits instead of sugar-sweetened beverages.
Limit foods with added sugars and HFCS.
Eat a balanced, nutrient-dense diet rich in vegetables, legumes, healthy fats, and lean protein.
Stay physically active.
Get sufficient sleep and manage stress.
If you have diabetes, liver disease, or other chronic conditions, consult your healthcare provider before starting a fasting regimen.
🔬 Bottom Line
Fasting may improve metabolic health and help counter some of the harmful effects of excessive fructose intake, but it is not a standalone cure. Reducing added sugars, maintaining a healthy diet, exercising regularly, and following evidence-based medical advice remain the most effective strategies for protecting long-term health.
===============================================================================================================================================================================================================================================================





Get in touch
Address
Cairo Al Rehab
Contacts
+20 109 405 2056
hassanalwarraqi@h-k-e-m.com