
Health is a crown on the heads of the healthy that only the sick can see.



🐝⚕️ Bee Venom vs Snakebite : Science vs Dangerous Myths
Discover what science really says about bee stings, snake venom, antivenom, cross-immunity myths, and emergency snakebite treatment.
AUTOIMMUNE DISEASESGENERAL
Dr Hassan Al Warraqi
5/12/202614 min read


🐝⚕️ Bee Venom vs Snakebite : Science vs Dangerous Myths
Discover what science really says about bee stings, snake venom, antivenom, cross-immunity myths, and emergency snakebite treatment.
Separating Dangerous Folk Beliefs from Proven Medicine
An evidence-based review of bee venom, the cross-immunity myth, and the only snakebite treatment that actually works
Introduction: The Persistent Folk Remedy That Can Kill
For centuries, traditional medicine systems across Asia, Africa, and the Americas have proposed natural antidotes for venomous snakebites.
Among the most persistent—and most dangerous—beliefs is that bee venom (apitoxin) can treat or even cure a snakebite.
This myth has survived through generations, fueled by anecdotal stories, cultural transmission, and a fundamental misunderstanding of how venom immunity works.
Beekeepers, folk healers, and online forums occasionally revive the claim that bee stings build cross-protection against snake venom—a notion that has never been validated by modern science.
When we examine the peer-reviewed scientific record, a clear and urgent conclusion emerges: Bee venom does not treat snakebites, and relying on it can be fatal.
This comprehensive review explains why the cross-immunity myth is false, explores the legitimate biomedical properties of bee venom, and gives you the only proven protocol for snakebite survival.
Snakebites Are Life-Threatening Medical Emergencies
Global Burden of Snakebite Envenoming
Venomous snakebites cause an estimated 81,000 to 138,000 deaths each year worldwide, according to the World Health Organization (WHO).
Hundreds of thousands more survivors suffer permanent disabilities, including:
Limb amputation (from necrosis)
Chronic kidney disease
Permanent neurological deficits
Loss of motor function
Psychological trauma
These are not minor injuries. A venomous snakebite is an acute toxic emergency that requires rapid, targeted medical intervention.
Why Snake Venom Is So Dangerous
Snake venoms are among the most biochemically complex substances in nature.
Depending on the species, venom may contain a cocktail of toxins:
Toxin Class
Primary Action
Clinical Consequence
Cytotoxins
Destroy local tissue
Necrosis, swelling, compartment syndrome
Hemotoxins
Disrupt blood clotting
Internal bleeding, thrombosis, stroke
Neurotoxins
Block nerve transmission
Respiratory paralysis, suffocation
Cardiotoxins
Damage heart muscle
Arrhythmia, cardiac arrest
Myotoxins
Destroy muscle tissue
Rhabdomyolysis, kidney failure
A single bite can trigger multi-organ failure within hours.
The clock starts ticking the moment fangs penetrate skin.
“Every minute between envenomation and antivenom administration is a minute that venom spends destroying tissue, disrupting coagulation, and potentially shutting down organ systems.”
— Consensus position, WHO Snakebite Initiative
The Only Proven Treatment: Antivenom
What Is Antivenom and How Is It Made?
Antivenom (also called antivenin or antivenom immunoglobulin) is produced by a carefully controlled process:
Immunization – Horses, sheep, or goats are injected with small, safe amounts of one or more snake venoms.
Antibody production – The animal’s immune system generates specific antibodies against each venom toxin.
Plasma collection – Antibody-rich plasma is harvested.
Purification – The plasma is processed to isolate immunoglobulins (mostly IgG and F(ab’)2 fragments).
Formulation – The purified antibodies are prepared for intravenous administration.
Antivenom remains the only clinically validated treatment capable of neutralizing circulating venom.
No other substance—natural or synthetic—has demonstrated equivalent efficacy in peer-reviewed clinical trials.
Why Antivenom Works
When injected into a snakebite victim, antivenom antibodies bind directly to venom toxins, forming complexes that are then cleared by the body’s immune system.
This neutralization:
Prevents further tissue damage
Restores normal blood coagulation
Reverses some neurotoxic effects (if given early)
Reduces mortality from ~30% to <1% in properly treated patients
✅ Medical Consensus: Antivenom is the sole evidence-based treatment for venomous snakebites. Its administration in a medical setting is irreplaceable.
No alternative therapy has been validated by clinical trial data.
Bee Venom: Genuinely Interesting, But Misapplied
What Bee Venom Actually Contains
Bee venom (apitoxin) is a legitimate subject of biomedical research.
It contains a complex mixture of bioactive compounds:
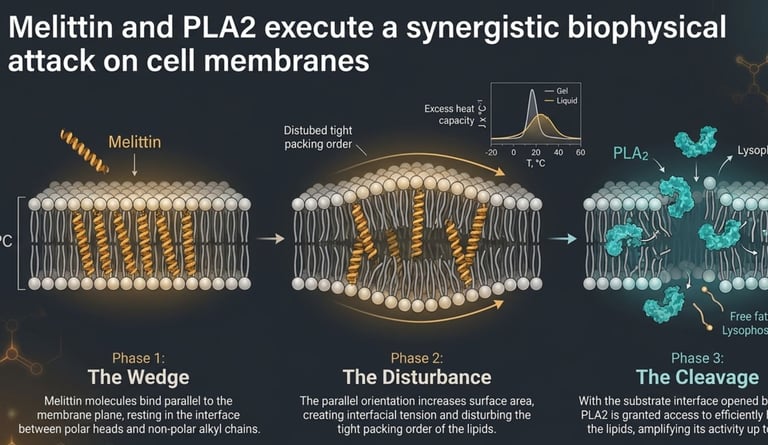
Melittin
40–60% of dry weight
Pore-forming peptide; anti-inflammatory, antimicrobial, antiviral potential
Phospholipase A2 (PLA2)
10–15%
Major allergen; hydrolyzes cell membranes; immunomodulatory
Hyaluronidase
1–2%
“Spreading factor” – helps venom diffuse through tissue
Apamin
2–3%
Neurotoxic peptide (specific to bees; not found in snake venom)
Mast cell degranulating peptide (MCDP)
1–2%
Histamine release; anti-inflammatory activity
Histamine, dopamine, other amines
Trace
Mediate pain, inflammation, and allergic response
Research has identified anti-inflammatory, antimicrobial, and even potential anticancer properties in bee venom components.
Apitherapy (the therapeutic use of bee products) is studied for conditions ranging from rheumatoid arthritis to neurological diseases like Parkinson’s. These are valid, ongoing areas of inquiry.
Where the Snakebite Claim Goes Wrong
The problem arises when preliminary laboratory findings are stretched into claims about snakebite treatment—a leap the evidence simply does not support.
Some in vitro (test tube) studies have found that melittin can inhibit the enzymatic activity of certain phospholipase A2 (PLA2) enzymes present in some snake venoms.
This is a real, interesting biochemical observation.
But several critical limitations apply:
In vitro (lab)
Melittin inhibits some PLA2 enzymes from certain vipers
Limited – no living system, no pharmacokinetics
Animal models
No consistent protective effect against whole venom
Not replicated or validated
Human clinical trials
None conducted
Zero evidence base
Antivenom trials
Consistent neutralization across species and toxin classes
Strongly supported
Why Lab Results Don’t Translate to Real Life
In vitro findings frequently fail to translate into clinical effectiveness because:
Metabolic breakdown – The human body rapidly degrades peptides like melittin via proteases.
Immune interference – Bee venom itself triggers an immune response that can complicate envenomation.
Distribution challenges – Melittin does not preferentially target snake venom toxins in the bloodstream; it is nonspecific.
Venom complexity – Snake venom contains dozens of distinct toxic compounds (enzymes, peptides, proteins, small molecules).
Inhibiting one enzyme in one venom type does not address the full spectrum of biological harm.
Dose mismatch – The amount of melittin needed to neutralize snake venom in vivo would likely be toxic and cause massive hemolysis.
⚠️ Important Distinction: A substance showing any interaction with a venom component in a petri dish is not the same as a substance that treats envenomation in a living patient.
This is one of the most commonly misunderstood gaps between research and medical application.
The Cross-Immunity Myth: Do Beekeepers Resist Snakebites?
One of the most widely circulated claims is that beekeepers—who are stung repeatedly over years—develop a kind of immunity that protects them from snakebites.
This idea has circulated in traditional communities for generations.
It sounds intuitive. It is not supported by evidence.
What Immunology Actually Says
Bee stings create general venom immunity
Immune responses are highly specific. Antibodies against bee venom do not recognize snake venom proteins.
Bee and snake venoms are similar
They share some superficial biochemical categories (both contain phospholipases) but differ vastly in protein sequence, three-dimensional structure, concentration, and mechanism of harm.
Anecdotes prove cross-immunity
Every report of a beekeeper surviving a snakebite is anecdotal. No control groups, no medical verification, no systematic data. Survivorship bias likely plays a major role.
Cross-reactivity occurs
Immunological cross-reactivity between bee and snake venoms has not been demonstrated at clinically meaningful levels. Antibody binding requires epitope matching—which does not exist here.
The Scientific Explanation
The antibodies a beekeeper develops are specific to bee venom antigens—proteins unique to Apis mellifera (or other bee species).
These antibodies belong to the IgG and IgE classes and recognize epitopes on melittin, PLA2, hyaluronidase, and other bee-specific peptides.
Snake venom toxins—such as snake PLA2, metalloproteinases, serine proteases, and three-finger toxins—have entirely different amino acid sequences and three-dimensional conformations.
No meaningful cross-binding occurs.
🔬 Bottom line: Cross-immunity between bee venom and snake venom is an unproven, biologically implausible concept.
Do not rely on it.
The Real Dangers of Pursuing Unproven Treatments
This is not merely a matter of ineffective treatment.
Relying on bee venom—or any folk remedy—after a snakebite creates its own cascade of dangers.
1. Delayed Antivenom Administration (The Most Lethal Risk)
Snake venom works fast:
Hemotoxic venoms (e.g., vipers, rattlesnakes) can trigger irreversible coagulopathy within 30–60 minutes.
Neurotoxic venoms (e.g., cobras, kraits, mambas) can impair breathing within 30–120 minutes.
Cytotoxic venoms can cause permanent tissue loss within hours.
Every minute spent attempting an alternative treatment is a minute of uncontested venom activity inside the body.
Delaying antivenom increases the risk of death or permanent disability exponentially.
2. Anaphylaxis from Bee Venom
Bee venom is a potent allergen.
Even individuals with no prior allergic history can develop severe anaphylaxis—especially when the immune system is already stressed by envenomation.
Anaphylaxis symptoms include:
Airway swelling (laryngeal edema)
Hypotension and shock
Urticaria and angioedema
Cardiovascular collapse
Introducing bee stings to a snakebite victim could trigger a second, simultaneous medical emergency, overwhelming an already compromised patient.
3. Additional Tissue Damage and Diagnostic Confusion
Multiple bee stings at or near the bite site cause local inflammation, pain, and tissue damage that can:
Mask the progression of snake venom symptoms
Mimic venom effects (swelling, redness, necrosis), confusing clinical assessment
Make treatment harder for emergency physicians
Increase the risk of secondary infection
4. False Reassurance
Perhaps the most insidious risk: performing a ritual of “treatment”—even an ineffective one—creates a psychological sense of having acted. This false reassurance can reduce the urgency the victim and bystanders feel about seeking real emergency care.
🚨 Critical Warning: None of the “folk remedies” are neutral—they are actively harmful. Cutting, sucking, ice, tourniquets, electric shock, alcohol, herbal poultices, and bee venom all worsen outcomes.
Correct Snakebite Response: What to Do and What Never to Do
Emergency medicine has clear, evidence-based protocols for snakebite response.
Following them correctly can mean the difference between full recovery and death or permanent disability.
✅ What To Do (Step by Step)
1
Stay calm and limit movement – Panic elevates heart rate and accelerates venom distribution. Keep the victim as still as possible.
2
Remove constricting items immediately – Remove watches, rings, bracelets, and tight clothing from the affected limb before swelling begins.
3
Immobilize the affected limb – Keep it at or below heart level. Use a splint or improvised support if available. Do not elevate above the heart.
4
Note the snake’s appearance (if safe) – Do not pursue or handle the snake. If possible, note size, color, pattern, and head shape to help medical staff select the correct antivenom.
5
Get to emergency medical care immediately – This is the single most important action. Do not wait for symptoms. Begin transport to the nearest hospital without delay. Call emergency services if available.
❌ What Never to Do (Actively Harmful)
Why It’s Dangerous
Suck out the venom
Introduces infection; removes negligible venom (less than 0.01% of injected dose)
Cut or incise the wound
Increases bleeding, infection, and tissue damage; may sever nerves or vessels
Apply ice or cold packs
Can accelerate tissue necrosis by vasoconstriction; no proven benefit
Apply a tourniquet
Concentrates venom damage; can cause limb loss, compartment syndrome, and reperfusion injury
Use electric shock
No benefit; causes burns, cardiac arrhythmia, and delays treatment
Apply bee venom or bee stings
Delays antivenom; risks anaphylaxis; adds tissue trauma
Drink alcohol
Worsens bleeding, impairs judgment, and accelerates venom absorption
Apply herbal poultices
Introduces infection; delays real treatment; may cause chemical burns
When Is Bee Venom Actually Used in Medicine?
To be clear: bee venom has legitimate medical applications—just not for snakebites.
Proven and Emerging Uses of Bee Venom Therapy (Apitherapy)
Rheumatoid arthritis
Mixed; some RCTs show mild benefit
Anti-inflammatory via melittin and PLA2; suppresses TNF-α, IL-1β
Osteoarthritis
Limited; needs more study
May reduce pain and swelling; unclear long-term efficacy
Multiple sclerosis
Preliminary; controversial
Immunomodulatory effects; some small trials show reduced lesion activity
Parkinson’s disease
Early animal studies
Neuroprotective potential via anti-inflammatory and anti-apoptotic pathways
Chronic pain (e.g., low back pain)
Limited
Melittin may desensitize nociceptors
Antiviral Research: A Promising Frontier
Emerging research shows that melittin and bee venom PLA2 have broad-spectrum antiviral activity in the lab:
HIV-1
Melittin inhibits viral transcription; bvPLA2 blocks entry via CXCR4 receptors
SARS-CoV-2
Modified melittin formulations (e.g., SIT-MEL complex) show potent inhibition in vitro
Influenza A (H1N1)
Melittin disrupts the viral envelope
Herpes simplex (HSV-1, HSV-2)
Inhibits viral attachment and entry
Enterovirus-71
Reduces viral RNA expression
⚠️ Important: These are laboratory findings, not clinical treatments.
No bee venom product is approved for treating viral infections in humans.
The same caution applies: in vitro success does not equal clinical medicine.
Why These Uses Don’t Translate to Snakebite Treatment
The antiviral and anti-inflammatory effects of bee venom are based on different mechanisms:
Disrupting lipid envelopes (viruses)
Modulating cytokines (inflammation)
Snake venoms are not viruses, and they are not simple inflammatory conditions.
They are complex mixtures of proteases, neurotoxins, and other enzymes that cause rapid, direct tissue destruction.
Neutralizing snake venom requires specific antibody binding to dozens of distinct toxin molecules—a task that melittin’s nonspecific membrane disruption cannot accomplish.
Scientific Verdict: Bee Venom for Snakebite
Peer-reviewed clinical trials
❌ None
Animal model protection
❌ Not demonstrated
Cross-immunity evidence
❌ Absent
Mechanism plausibility
❌ Low (melittin inhibits only some PLA2 enzymes in vitro; irrelevant for whole venom)
Safety in snakebite context
❌ Dangerous (anaphylaxis, delay, tissue damage)
Antivenom comparison
✅ Antivenom is the only proven treatment
Conclusion: Bee venom has not been shown to treat snakebites in any clinical or peer-reviewed setting.
The idea is a dangerous myth.
Why Bee Venom Is Never a Rational “Last Resort”
Even when antivenom is out of reach, bee venom fails as a rescue treatment for four fatal reasons:
1. It Does Not Neutralize Snake Venom
Bee venom contains melittin, which in a test tube can inhibit one class of enzymes (certain phospholipase A2) found in some snake venoms.
But snake venom contains dozens of different toxins: metalloproteinases, serine proteases, neurotoxins, cardiotoxins, myotoxins, etc. Melittin does nothing against the vast majority of these.
It is like trying to stop a car by blocking one spark plug—the engine keeps running.
In animal studies, bee venom has never shown consistent protection against whole-venom envenomation.
No living snakebite victim has ever been saved by bee venom.
2. It Can Kill You Faster
A snakebite already stresses your body. Adding bee venom—especially multiple stings—risks:
Immediate anaphylaxis (closing airways, crashing blood pressure)
Additional tissue necrosis at the sting sites
Immune system overload, accelerating venom spread
You would be trading one poison for another, with no neutralizing benefit.
3. It Wastes Precious Time
Every minute spent applying bees or bee venom is a minute not spent on supportive care—the only thing that might help when antivenom is absent.
That time loss is irreversible.
4. It Gives False Hope
Believing you have “done something” often stops people from seeking other help or continuing basic life support.
That false reassurance is deadly.
What Actually Works When Antivenom Is Unavailable?
If you are in a remote setting with no antivenom (and no possibility of evacuation), the goal shifts from neutralizing venom to supporting vital functions until your body can slowly clear the venom on its own (which takes days to weeks).
This is called supportive care, and it is what doctors did before antivenom existed.
Evidence-Based Last-Resort Measures (No Bee Venom)
Keep victim completely still
Reduces venom spread via lymphatics
Immobilize the bitten limb at or below heart level
Slows systemic absorption
Remove all tight items (rings, watches, clothing)
Prevents constriction as swelling occurs
Monitor breathing
If neurotoxic venom (cobra, krait, mamba), prepare to do mouth-to-mouth or bag-valve ventilation for hours or days until venom wears off
Treat pain (if available: oral acetaminophen/paracetamol; avoid NSAIDs like ibuprofen if bleeding risk)
Reduces stress and heart rate
Keep victim warm and hydrated (if able to swallow safely)
Prevents shock
Do NOT give alcohol, aspirin, or sedatives
Worsens bleeding or breathing depression
In a Hospital Without Antivenom (Low-Resource Setting)
Even without specific antivenom, hospitals can provide:
Mechanical ventilation for neurotoxic paralysis (this saves lives—krait and cobra victims can survive if ventilated for 1–2 weeks)
Blood transfusions for bleeding disorders (viper bites)
Dialysis for kidney failure
Wound care and debridement for necrosis
These supportive measures reduce mortality significantly compared to doing nothing—or using harmful folk remedies.
The Only Scenario Where Bee Venom Is Considered in Medicine (Not Snakebite)
Bee venom is studied for:
Rheumatoid arthritis (anti-inflammatory)
Some viral infections (lab only)
Desensitization for bee-allergic patients
None of these involve snakebite. There is no peer-reviewed protocol, no case report, no clinical trial where bee venom improved snakebite outcome.
Final Verdict: Do Not Use Bee Venom for Snakebite, Ever
Situation
What to Do
Antivenom available
Go to hospital immediately. Antivenom is the only cure.
Antivenom not available, but hospital reachable
Go to hospital anyway for supportive care (ventilation, blood products, dialysis).
Antivenom not available, no hospital possible
Use supportive care (immobilization, breathing support, hydration). Do not use bee venom, herbs, electric shock, tourniquets, or cuts.
Frequently Asked Questions (FAQ)
❓ Can bee venom cure a snakebite?
No.
There is no scientific evidence that bee venom cures or treats snakebites.
The only proven treatment is antivenom administered in a hospital.
❓ Do beekeepers have immunity to snakebites?
No.
Beekeepers develop immunity only to bee venom.
Their antibodies do not recognize snake venom proteins.
This is a persistent myth with no scientific basis.
❓ What is antivenom and how does it work?
Antivenom is made by immunizing horses or sheep with snake venom.
The animals produce antibodies that are harvested and purified.
When injected into a snakebite victim, these antibodies bind to and neutralize snake venom toxins.
❓ What should I do immediately after a snakebite?
Stay calm, immobilize the limb, remove tight items, and get to a hospital immediately.
Do not attempt any home remedies. Time is critical.
❓ Is bee venom therapy (apitherapy) ever medically valid?
Yes,
for specific conditions like arthritis and possibly certain viral infections in research settings.
However, it is not validated for snakebites, and using it for that purpose is dangerous.
❓ Why is bee venom dangerous for snakebite victims specifically?
Because it can:
Delay life-saving antivenom administration
Trigger anaphylaxis (a second emergency)
Cause additional tissue damage
Provide false reassurance, reducing urgency to seek real care
❓ How quickly does snake venom act?
Very quickly.
Hemotoxic venoms can cause bleeding disorders within 30–60 minutes. Neurotoxic venoms can paralyze breathing within 1–2 hours.
Cytotoxic venoms can cause permanent tissue loss in hours. Every minute matters.
❓ Are there ongoing research efforts to develop better snakebite treatments?
Yes.
Researchers are exploring:
New antivenom formulations (e.g., synthetic antibodies, small molecule inhibitors)
Improved cold-chain stability for tropical regions
Oral or subcutaneous delivery methods
Plant-derived inhibitors (e.g., from Mimosa pudica, Eclipta prostrata)
But none of these involve bee venom as a substitute for antivenom.
Key Facts Summary
Global snakebite deaths per year
81,000–138,000 (WHO estimate)
Only proven treatment
Antivenom (immunoglobulin from immunized animals)
Clinical trials of bee venom for snakebite
Zero
Cross-immunity between bee and snake venom
Unproven (no scientific evidence)
Bee venom anaphylaxis risk
High, even without prior allergy
Time window for effective antivenom
Minutes to a few hours (depends on venom type)
Major complications without antivenom
Hemorrhage, paralysis, kidney failure, death
🚨 In an Emergency: Snakebite First Aid Card
If bitten by a snake:
Stay calm – panic spreads venom faster.
Minimize movement – keep the victim still.
Remove tight items (rings, watches, bracelets).
Immobilize the limb at or below heart level.
Go to a hospital NOW – call emergency services or drive.
Do NOT attempt:
✗ Sucking or cutting the wound
✗ Ice, tourniquets, or electric shock
✗ Alcohol, herbs, or bee venom
Time is the most critical factor. Nothing else helps.
==============================================================================================================================================================================================
🐝⚕️ Bee Venom vs Snakebite : Science vs Dangerous Myths
Bee venom does not cure snakebites, and there is no scientific evidence that bee stings can neutralize snake venom.
While bee venom is being researched for anti-inflammatory and antiviral effects, it is not a substitute for antivenom — the only proven treatment for venomous snakebites.
Dangerous myths about bee venom, cutting wounds, sucking venom, or herbal remedies can delay life-saving medical care and increase the risk of paralysis, organ failure, or death.
✅ Correct response to a snakebite:
Stay calm
Immobilize the limb
Remove tight items
Seek emergency medical care immediately
❌ Never use:
Bee stings or bee venom
Ice or tourniquets
Cutting or sucking the wound
Alcohol or electric shock
🚑 Time and antivenom save lives.
bee venom vs snakebite, bee venom snakebite myth, can bee venom cure snakebite, snakebite treatment, antivenom therapy, bee stings and snake venom, snake venom immunity myth, bee venom science, apitherapy snakebite, dangerous snakebite remedies, venom cross immunity, snakebite first aid, bee venom therapy, venomous snakebite emergency, antivenom facts, snakebite medical treatment, melittin snake venom, bee venom research, toxicology myths, emergency snakebite care
#BeeVenom #Snakebite #Antivenom #SnakeVenom #MedicalMyths #ScienceVsMyth #EmergencyMedicine #Toxicology #Apitherapy #SnakebiteTreatment #HealthEducation #EvidenceBasedMedicine #VenomResearch #FirstAid #MedicalFacts #MythBusting #PublicHealth #PoisonControl #BeeStings #SurvivalFacts
==============================================================================================================================================================================================
🛡️ Fasting & Cancer Prevention: Myth or Medical Reality?
⚡ Short Summary (2026 Evidence)
The short answer: Not a myth—but not a magic shield either.
Fasting shows promising biological mechanisms for cancer prevention in lab studies, but human evidence is still emerging.
It's a potential adjunct tool, not a standalone cure or guarantee.
🔬 What the Science Says (2026)
✅ Supported Mechanisms (Preclinical Data):
Mechanism
How It May Help
Evidence Level
Reduced IGF-1
Lower insulin-like growth factor = slower tumor growth
Strong (animal/human biomarker)
Autophagy Activation
Clears damaged cells before they become cancerous
Strong (cell/animal); emerging (human)
Lower Inflammation
Chronic inflammation drives cancer; fasting reduces markers like CRP, IL-6
Moderate (human trials)
Metabolic Switching
Ketones may starve some cancer cells that rely on glucose
Promising (lab); limited (human)
Improved Insulin Sensitivity
High insulin/obesity = cancer risk; fasting improves both
Strong (human metabolic data)
⚠️ Human Evidence Status:
Observational studies: Intermittent fasting linked to lower breast, colorectal cancer risk—but correlation ≠ causation.
Clinical trials: Small studies show fasting during chemotherapy may reduce side effects and improve tolerance.
Prevention trials: No large-scale RCTs yet proving fasting prevents cancer in humans.
2026 consensus: Biologically plausible, but not yet proven as a standalone prevention strategy.
🎯 Practical Takeaway
✅ What You Can Do Today:
Time-restricted eating (12–16 hr window): Safe for most; supports metabolic health (a known cancer risk reducer).
Combine with proven strategies: Whole-food diet, exercise, sleep, avoid smoking/alcohol, regular screenings.
If undergoing cancer treatment: Discuss fasting only with your oncology team—never self-prescribe.
❌ What Not to Do:
Don't replace screenings or treatment with fasting.
Don't attempt prolonged fasts (>48h) without medical supervision.
Don't believe claims that fasting "starves cancer" alone—it's far more complex.
🚫 Who Should Avoid Fasting for Cancer Prevention:
Active cancer patients (unless under oncology supervision)
History of eating disorders
Underweight or malnourished individuals
Pregnant/breastfeeding women
Type 1 diabetes or advanced Type 2 diabetes
🧭 Bottom Line (2026)
🛡️ Fasting is a promising piece of the cancer prevention puzzle—but not the whole picture.
🔬 Mechanisms are real; human proof is pending.
🎯 Best use: As part of a holistic, evidence-based lifestyle—not a standalone shield.
When in doubt: Prioritize proven prevention (screenings, healthy weight, no tobacco) and discuss fasting with your doctor.
🔍 SEO Keywords: fasting cancer prevention 2026, intermittent fasting oncology, autophagy cancer research, IGF-1 fasting, metabolic health cancer risk
==============================================================================================================================================================================================






Get in touch
Address
Cairo Al Rehab
Contacts
+20 109 405 2056
hassanalwarraqi@h-k-e-m.com